Sharma Rakesh K, Voelker Donald J, Sharma Rohit, Reddy Hanumanth K, Dod Harvinder, Marsh James D
Medical Center of South Arkansas, Heart and Vascular Institute, 700 West Grove Street, El Dorado, AR 71730, USA.
Vasc Health Risk Manag. 2012;8:65-75. doi: 10.2147/VHRM.S28090. Epub 2012 Feb 8.
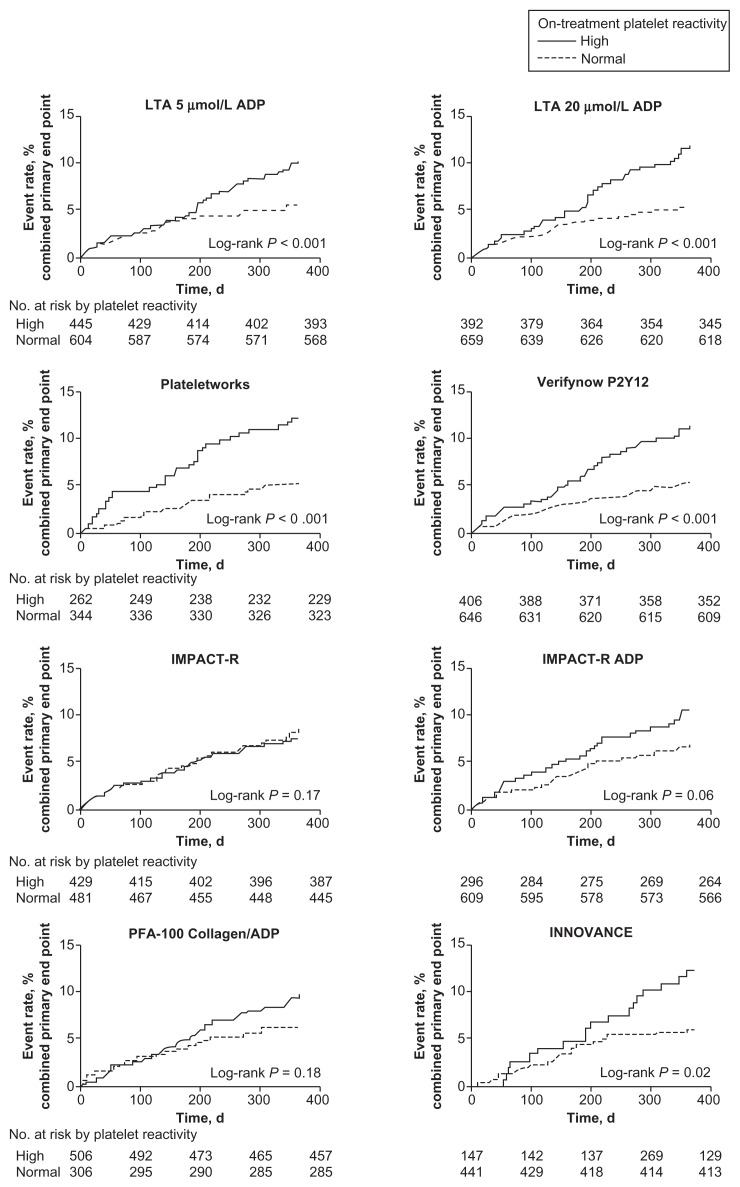
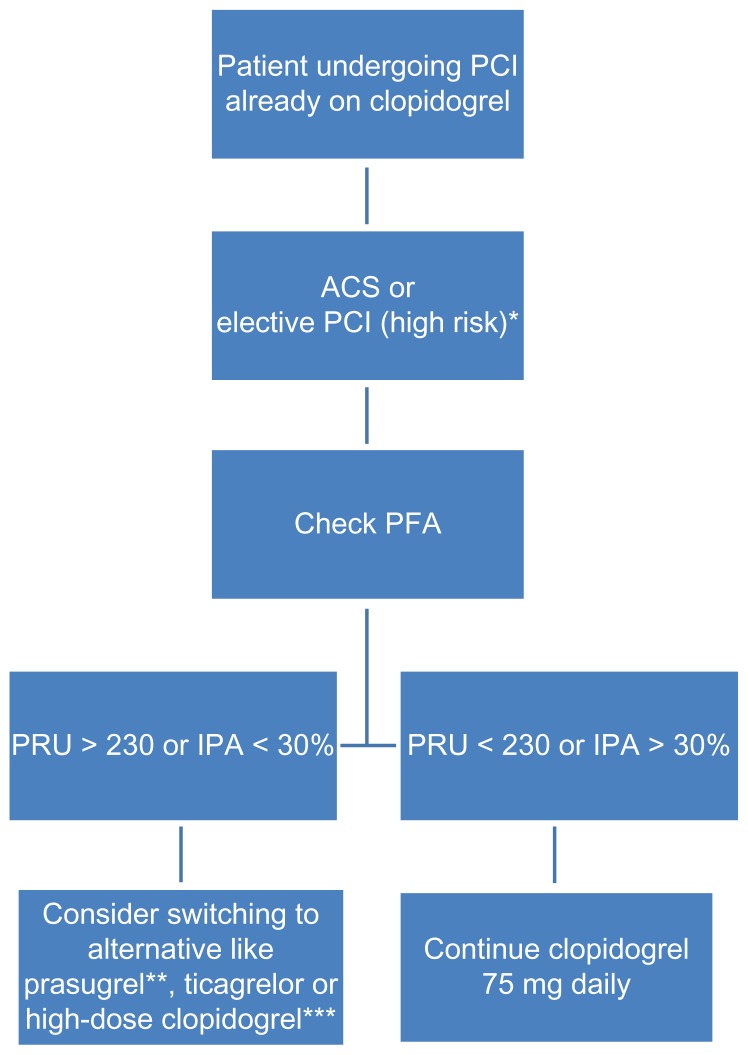
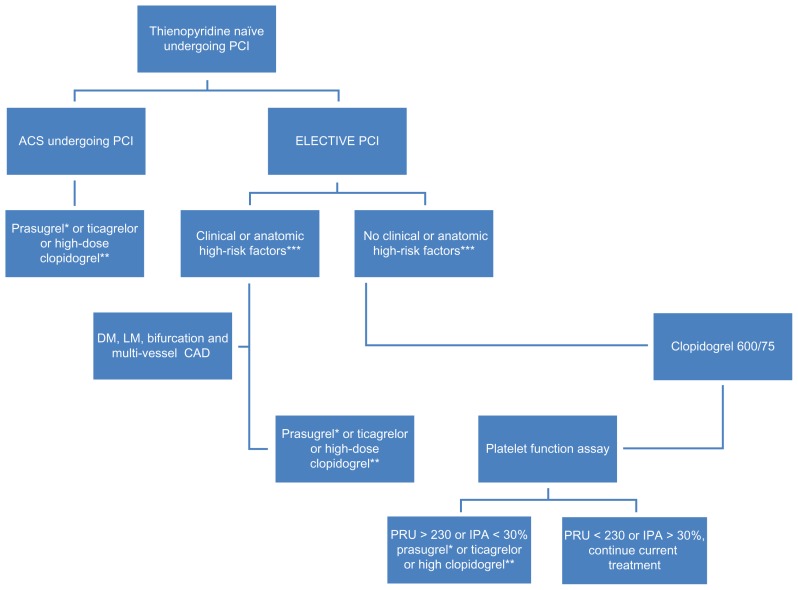
The substantial reduction in ischemic events provided by the dual antiplatelet regimen with aspirin and clopidogrel is well documented in patients with acute coronary syndrome and patients undergoing percutaneous coronary intervention. Recently the variable response to the antiplatelet agents has received considerable attention after several "boxed warnings" on clopidogrel. This led to intense controversy on pharmacokinetic, pharmacodynamic, and pharmacogenomic issues of antiplatelet drugs, especially clopidogrel. Research use of platelet function testing has been successfully validated in identifying new antiplatelet drugs like prasugrel and ticagrelor. These platelet function assays are no longer regarded just as a laboratory phenomenon but rather as tools that have been shown to predict mortality in several clinical trials. It is believed that suboptimal response to an antiplatelet regimen (pharmacodynamic effect) may be associated with cardiovascular, cerebrovascular, and peripheral arterial events. There has been intense controversy about this variable response of antiplatelet drugs and the role of platelet function testing to guide antiplatelet therapy. While the importance of routine platelet function testing may be uncertain, it may be useful in high-risk patients such as those with diabetes mellitus, diffuse three vessels coronary artery disease, left main stenosis, diffuse atherosclerotic disease, and those with chronic renal failure undergoing percutaneous coronary intervention. It could also be useful in patients with suspected pharmacodynamic interaction with other drugs to assure the adequacy of platelet inhibition. While we wait for definitive trials, a predictive prognostic algorithm is necessary to individualize antiplatelet therapy with P2Y12 inhibitors based on platelet function assays and genetic testing.
阿司匹林和氯吡格雷双重抗血小板治疗方案能显著降低缺血事件的发生,这在急性冠脉综合征患者和接受经皮冠状动脉介入治疗的患者中已有充分记录。最近,在氯吡格雷发布多个“黑框警告”后,抗血小板药物的个体反应差异受到了广泛关注。这引发了关于抗血小板药物,尤其是氯吡格雷的药代动力学、药效学和药物基因组学问题的激烈争论。血小板功能检测在研究中已成功验证可用于识别新型抗血小板药物,如普拉格雷和替格瑞洛。这些血小板功能检测不再仅仅被视为一种实验室现象,而是已被证明能在多项临床试验中预测死亡率的工具。人们认为,抗血小板治疗方案的反应欠佳(药效学效应)可能与心血管、脑血管和外周动脉事件相关。关于抗血小板药物的这种个体反应差异以及血小板功能检测在指导抗血小板治疗中的作用,一直存在激烈争论。虽然常规血小板功能检测的重要性可能尚不明确,但在高危患者中可能有用,如糖尿病患者、弥漫性三支血管冠状动脉疾病患者、左主干狭窄患者、弥漫性动脉粥样硬化疾病患者以及接受经皮冠状动脉介入治疗的慢性肾衰竭患者。对于怀疑与其他药物存在药效学相互作用的患者,检测也有助于确保血小板抑制的充分性。在等待确定性试验结果的同时,需要一种预测性的预后算法,以便根据血小板功能检测和基因检测结果,对使用P2Y12抑制剂的抗血小板治疗进行个体化调整。