Department of Medicine, McMaster University, Hamilton, Ontario, Canada.
Diabetes Care. 2012 Apr;35(4):787-93. doi: 10.2337/dc11-1855. Epub 2012 Feb 28.
Self-management of type 2 diabetes including avoidance of hypoglycemia is complex, but the impact of cognition on safe self-management is not well understood. This study aimed to assess the effect of baseline cognitive function and cognitive decline on subsequent risk of severe hypoglycemia and to assess the effect of different glycemic strategies on these relationships.
Prospective cohort analysis of data from the ACCORD trial included 2,956 adults aged ≥55 years with type 2 diabetes and additional cardiovascular risk factors. Cognitive tests (Digit Symbol Substitution Test [DSST], Rey Auditory Verbal Learning Test, Stroop Test, and Mini Mental Status Examination) were conducted at baseline and 20 months. Study outcomes were incident confirmed severe hypoglycemia requiring medical assistance (HMA) and hypoglycemia requiring any assistance (HAA).
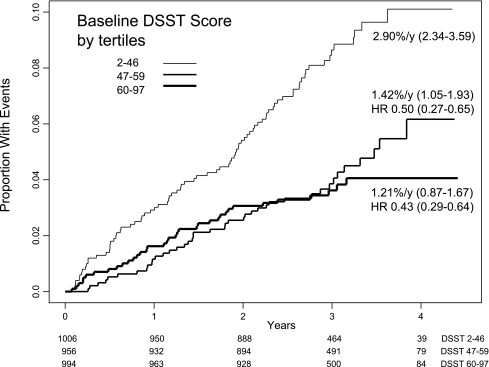
After a median 3.25-year follow-up, a 5-point-poorer baseline score on the DSST was predictive of a first episode of HMA (hazard ratio 1.13 [95% CI 1.08-1.18]). Analyses of the other cognitive tests and of HAA were consistent with the DSST results. Cognitive decline over 20 months increased the risk of subsequent hypoglycemia to a greater extent in those with lower baseline cognitive function (P(interaction) = 0.037). Randomization to an intensive versus standard glycemic strategy had no impact on the relationship between cognitive function and the risk of severe hypoglycemia.
Poor cognitive function increases the risk of severe hypoglycemia in patients with type 2 diabetes. Clinicians should consider cognitive function in assessing and guiding their patients regarding safe diabetes self-management regardless of their glycemic targets.
2 型糖尿病的自我管理(包括避免低血糖)较为复杂,但认知对安全自我管理的影响尚未被充分了解。本研究旨在评估基线认知功能和认知下降对随后严重低血糖风险的影响,并评估不同血糖控制策略对这些关系的影响。
ACCORD 试验的前瞻性队列分析纳入了 2956 名年龄≥55 岁、患有 2 型糖尿病且伴有其他心血管危险因素的成年人。在基线和 20 个月时进行认知测试(数字符号替换测试[DSST]、 Rey 听觉言语学习测试、Stroop 测试和简易精神状态检查)。研究结局为首次确诊需要医疗协助的严重低血糖(HMA)和需要任何协助的低血糖(HAA)。
中位随访 3.25 年后,DSST 基线评分每下降 5 分,首次发生 HMA 的风险比为 1.13(95%CI 1.08-1.18)。对其他认知测试和 HAA 的分析结果与 DSST 结果一致。在认知功能较差的患者中,20 个月内认知功能下降与随后低血糖风险增加之间的相关性更大(P(交互作用)=0.037)。与标准血糖控制策略相比,强化血糖控制策略对认知功能与严重低血糖风险之间的关系没有影响。
认知功能较差会增加 2 型糖尿病患者发生严重低血糖的风险。无论血糖控制目标如何,临床医生在评估和指导患者安全进行糖尿病自我管理时都应考虑认知功能。