Intensive Care Unit, Poliambulanza Hospital Foundation, Brescia, Italy.
BMC Anesthesiol. 2012 Mar 5;12:3. doi: 10.1186/1471-2253-12-3.
Mean arterial pressure above 65 mmHg is recommended for critically ill hypotensive patients whereas they do not benefit from supranormal cardiac output values. In this study we investigated if the increase of mean arterial pressure after volume expansion could be predicted by cardiovascular and renal variables. This is a relevant topic because unnecessary positive fluid balance increases mortality, organ dysfunction and Intensive Care Unit length of stay.
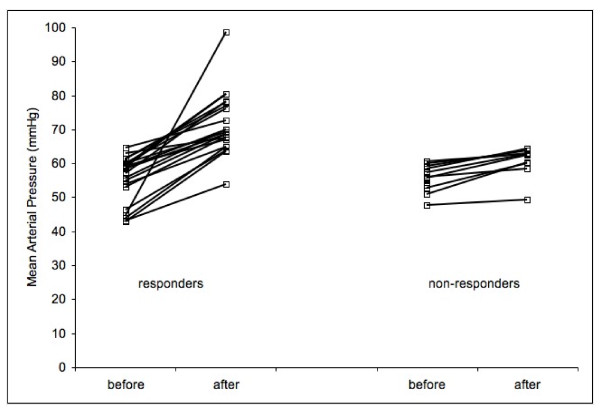
Thirty-six hypotensive patients (mean arterial pressure < 65 mmH) received a fluid challenge with hydroxyethyl starch. Patients were excluded if they had active bleeding and/or required changes in vasoactive agents infusion rate in the previous 30 minutes. Responders were defined by the increase of mean arterial pressure value to over 65 mmHg or by more than 20% with respect to the value recorded before fluid challenge. Measurements were performed before and at one hour after the end of fluid challenge.
Twenty-two patients (61%) increased arterial pressure after volume expansion. Baseline heart rate, arterial pressure, central venous pressure, central venous saturation, central venous to arterial PCO2 difference, lactate, urinary output, fractional excretion of sodium and urinary sodium/potassium ratio were similar between responder and non-responder. Only 7 out of 36 patients had valuable dynamic indices and then we excluded them from analysis. When the variables were tested as predictors of responders, they showed values of areas under the ROC curve ranging between 0.502 and 0.604. Logistic regression did not reveal any association between variables and responder definition.
Fluid challenge did not improve arterial pressure in about one third of hypotensive critically ill patients. Cardiovascular and renal variables did not enable us to predict the individual response to volume administration.
ClinicalTrials.gov: NCT00721604.
对于低血压危重症患者,推荐将平均动脉压维持在 65mmHg 以上,而高于正常的心输出量并不能使他们获益。本研究旨在探讨在容量复苏后,平均动脉压的升高是否可以通过心血管和肾功能变量来预测。这是一个非常重要的课题,因为不必要的正液平衡会增加死亡率、器官功能障碍和 ICU 住院时间。
36 例低血压(平均动脉压 < 65mmHg)患者接受羟乙基淀粉的容量负荷试验。如果患者有活动性出血或在过去 30 分钟内需要改变血管活性药物输注速度,则将其排除。通过平均动脉压升高超过 65mmHg 或与容量负荷试验前相比升高超过 20%来定义为有反应者。在容量负荷试验前和结束后 1 小时进行测量。
22 例(61%)患者在容量复苏后动脉压升高。反应者和无反应者的基线心率、动脉压、中心静脉压、中心静脉饱和度、中心静脉与动脉 PCO2 差值、乳酸、尿量、钠排泄分数和尿钠/钾比值相似。只有 36 例患者中的 7 例有有价值的动态指标,因此将其排除在分析之外。当将这些变量作为反应者的预测因子进行测试时,它们的 ROC 曲线下面积在 0.502 到 0.604 之间。逻辑回归未发现变量与反应者定义之间的任何关联。
大约三分之一的低血压危重症患者的动脉压在容量负荷试验后并未改善。心血管和肾功能变量不能帮助我们预测对容量治疗的个体反应。
ClinicalTrials.gov:NCT00721604。