Verma Sanjeev Kumar, Maheshwari Sandhya, Sharma Naresh Kumar, Prabhat K C
Department of Orthodontics and Dental Anatomy, Dr. Z. A. Dental College, Aligarh Muslim University, Aligarh, India.
Natl J Maxillofac Surg. 2010 Jan;1(1):35-40. doi: 10.4103/0975-5950.69162.
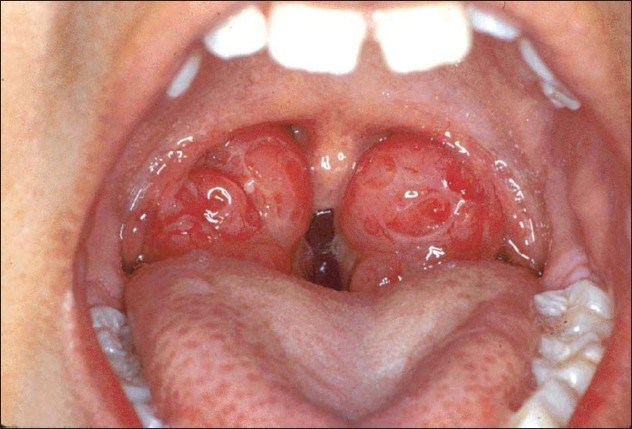
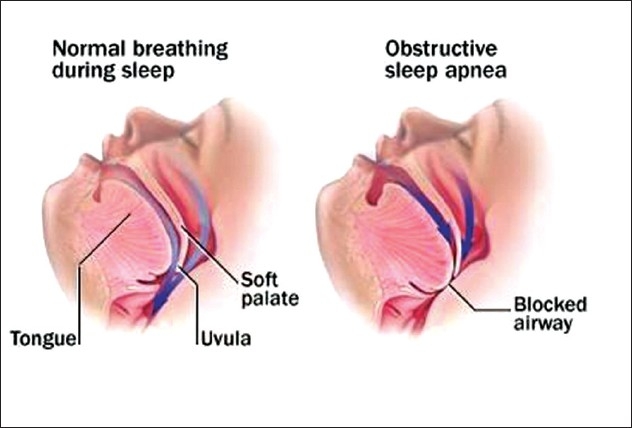
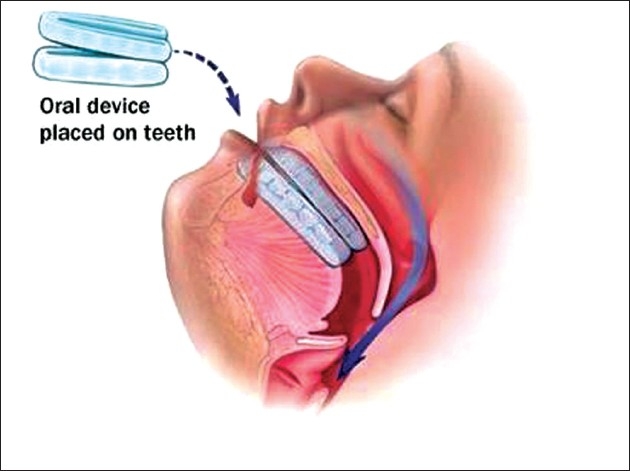
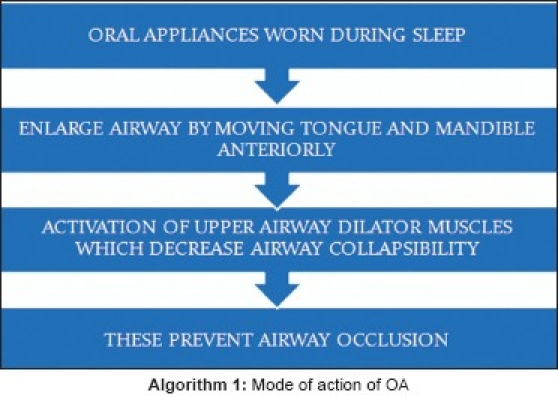
Sleep disordered breathing (SDB) in children is common. The impact of SDB on the growth and development of child may have detrimental effects on health, neuropsychological development, quality of life, and economic potential; therefore, SDB in children should be recognized as a public health problem as in the adult population. The coexistence of obesity and obstructive sleep apnea (OSA) not only appears to yield increased morbidity rates and poorer responses to therapy, but also is altogether associated with a distinct and recognizable clinical phenotype. Therapeutic options have somewhat expanded since the initial treatment approaches were conducted, to include not only surgical extraction of hypertrophic adenoids and tonsils, but also nonsurgical alternatives such as continuous positive air pressure, anti-inflammatory agents and oral appliances (OAs). Now, American academy of sleep medicine (AAOSM) has recommended OAs for OSA, hence the therapeutic interventions that are directed at the site of airway obstruction in the maxillofacial region are within the scope of dentistry. Among the physicians treating the children, dentists are more likely to identify adenotonsillar hypertrophy. Hence, the dentist can play an important role in identifying and treating those cases with OAs, who refuse the surgery, or those with structural abnormality in which myofunctional appliances are beneficial.
儿童睡眠呼吸障碍(SDB)很常见。SDB对儿童生长发育的影响可能会对健康、神经心理发育、生活质量和经济潜力产生不利影响;因此,儿童SDB应像成人一样被视为一个公共卫生问题。肥胖与阻塞性睡眠呼吸暂停(OSA)并存不仅似乎会导致发病率增加和对治疗的反应较差,而且还与一种独特且可识别的临床表型相关。自从最初的治疗方法实施以来,治疗选择有所扩展,不仅包括手术切除肥大的腺样体和扁桃体,还包括非手术替代方法,如持续气道正压通气、抗炎药物和口腔矫治器(OAs)。现在,美国睡眠医学学会(AAOSM)已推荐使用OAs治疗OSA,因此针对颌面区域气道阻塞部位的治疗干预属于牙科范畴。在治疗儿童的医生中,牙医更有可能识别出腺样体扁桃体肥大。因此,牙医在识别和治疗那些拒绝手术的OSA病例或肌功能矫治器有益的结构异常病例方面可以发挥重要作用。