Garbati Musa A, Ahsan Azeem M, Hakawi Ahmed M
Division of Infectious Diseases, Department of Medicine, King Fahad Medical City, 11525, Riyadh, Saudi Arabia.
J Med Case Rep. 2012 Apr 3;6:97. doi: 10.1186/1752-1947-6-97.
Lemierre's syndrome was originally documented to be caused by Fusobacterium necrophorum. It is a very rare condition with a prevalence of one to 14.4 instances per million. Its presentation is varied, not only in composition but also in the infecting organism. Treatment with anticoagulants has been controversial and applied only on a case-by-case basis.
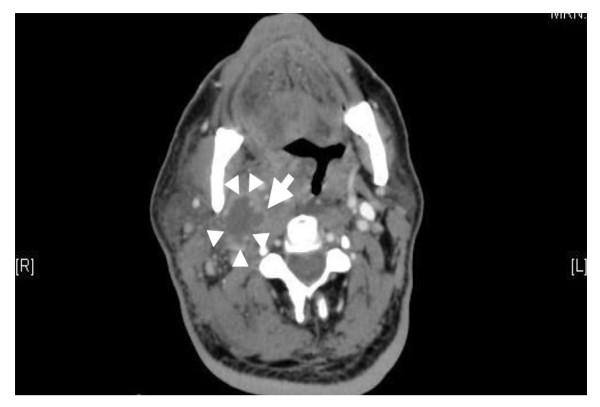
A 63-year-old Saudi man who had had uncontrolled diabetes mellitus for 47 years presented to our facility with a five-day history of swelling on the right side of his neck and fever. The swelling progressively increased in size and was associated with pain, dysphagia, odynophagia, change of voice ('hot potato voice'), and reduced appetite. Abscess content culture and sensitivity testing revealed Klebsiella pneumoniae. However, blood culture results were repeatedly negative. The abscess was incised and drained without any complication. Our patient was treated with clindamycin and cefuroxime. Warfarin was also administered concurrently for six weeks, for an isolated internal jugular vein thrombosis (IJV), with complete resolution of the thrombus. Normoglycemia was achieved and our patient was discharged after complete wound healing and the return of his biochemical parameters to normal.
Only two cases of Lemierre's syndrome in patients with diabetes due to K. pneumoniae have been reported previously. A review of the literature suggested that an association exists between deep neck infections due to K. pneumoniae and diabetes mellitus. The reasons for this association are still not clear. This poses a question as to whether diabetes mellitus specifically predisposes these patients to infection with this organism. It is suggested that clinicians should consider infectious agents other than F. necrophorum in the causation of Lemierre's syndrome, especially in patients with diabetes.
勒米尔综合征最初被记录为由坏死梭杆菌引起。这是一种非常罕见的疾病,每百万例中患病率为1至14.4例。其表现形式多样,不仅在构成上,而且在感染病原体方面。抗凝治疗一直存在争议,仅根据具体病例应用。
一名63岁的沙特男子,患有47年未得到控制的糖尿病,因右侧颈部肿胀和发热5天前来我院就诊。肿胀逐渐增大,并伴有疼痛、吞咽困难、吞咽痛、声音改变(“热土豆音”)和食欲减退。脓肿内容物培养及药敏试验显示为肺炎克雷伯菌。然而,血培养结果多次为阴性。脓肿切开引流,无任何并发症。我们的患者接受了克林霉素和头孢呋辛治疗。同时还给予华法林治疗6周,用于孤立性颈内静脉血栓形成,血栓完全溶解。血糖恢复正常,患者在伤口完全愈合且生化指标恢复正常后出院。
此前仅报道过2例糖尿病患者因肺炎克雷伯菌引起的勒米尔综合征。文献综述表明,肺炎克雷伯菌引起的颈部深部感染与糖尿病之间存在关联。这种关联的原因尚不清楚。这就提出了一个问题,即糖尿病是否特别使这些患者易感染这种病原体。建议临床医生在勒米尔综合征的病因中应考虑坏死梭杆菌以外的感染病原体,尤其是糖尿病患者。