Department of Bioengineering, The Institute of Engineering in Medicine, University of California, San Diego, La Jolla, California, United States of America.
PLoS One. 2012;7(3):e32672. doi: 10.1371/journal.pone.0032672. Epub 2012 Mar 27.
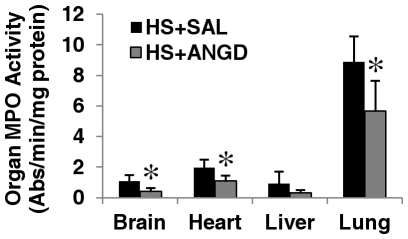
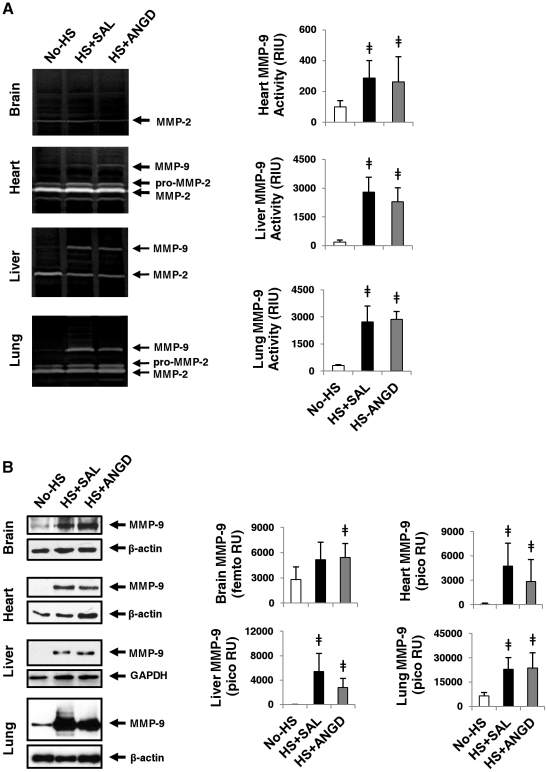
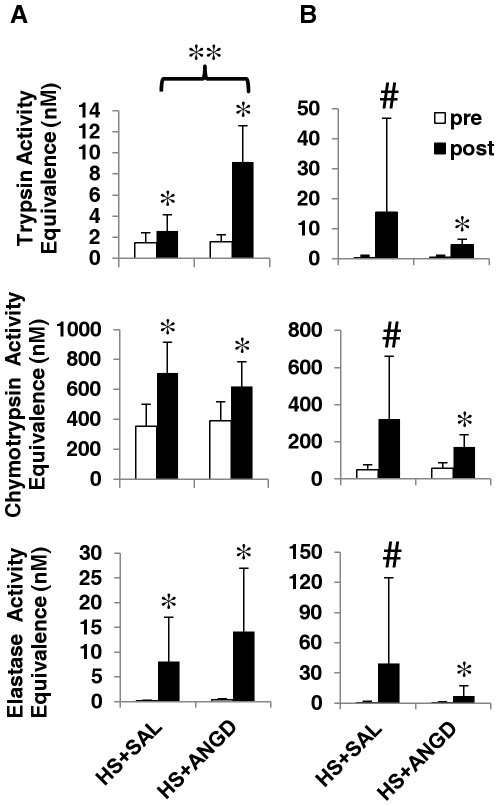
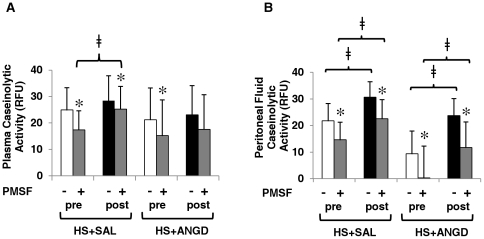
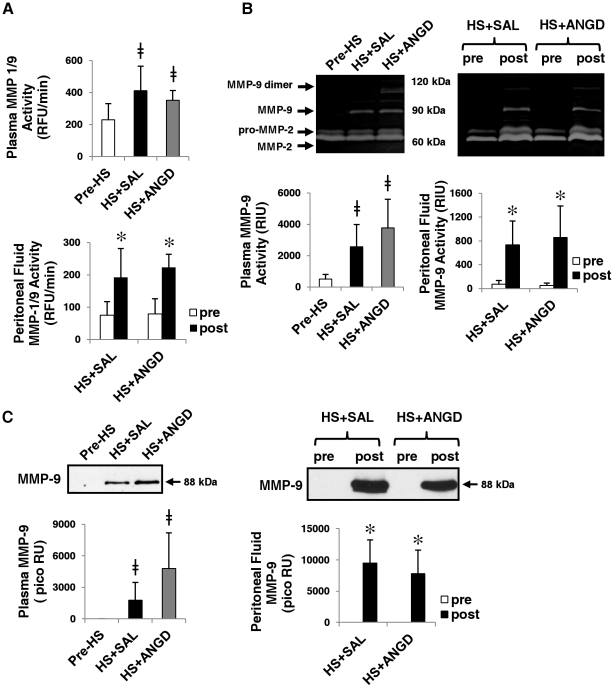
Hemorrhagic shock (HS) is associated with high mortality. A severe decrease in blood pressure causes the intestine, a major site of digestive enzymes, to become permeable - possibly releasing those enzymes into the circulation and peritoneal space, where they may in turn activate other enzymes, e.g. matrix metalloproteinases (MMPs). If uncontrolled, these enzymes may result in pathophysiologic cleavage of receptors or plasma proteins. Our first objective was to determine, in compartments outside of the intestine (plasma, peritoneal fluid, brain, heart, liver, and lung) protease activities and select protease concentrations after hemorrhagic shock (2 hours ischemia, 2 hours reperfusion). Our second objective was to determine whether inhibition of proteases in the intestinal lumen with a serine protease inhibitor (ANGD), a process that improves survival after shock in rats, reduces the protease activities distant from the intestine. To determine the protease activity, plasma and peritoneal fluid were incubated with small peptide substrates for trypsin-, chymotrypsin-, and elastase-like activities or with casein, a substrate cleaved by multiple proteases. Gelatinase activities were determined by gelatin gel zymography and a specific MMP-9 substrate. Immunoblotting was used to confirm elevated pancreatic trypsin in plasma, peritoneal fluid, and lung and MMP-9 concentrations in all samples after hemorrhagic shock. Caseinolytic, trypsin-, chymotrypsin-, elastase-like, and MMP-9 activities were all significantly (p<0.05) upregulated after hemorrhagic shock regardless of enteral pretreatment with ANGD. Pancreatic trypsin was detected by immunoblot in the plasma, peritoneal space, and lungs after hemorrhagic shock. MMP-9 concentrations and activities were significantly upregulated after hemorrhagic shock in plasma, peritoneal fluid, heart, liver, and lung. These results indicate that protease activities, including that of trypsin, increase in sites distant from the intestine after hemorrhagic shock. Proteases, including pancreatic proteases, may be shock mediators and potential targets for therapy in shock.
失血性休克(HS)与高死亡率相关。血压严重下降会导致肠道(消化酶的主要部位)变得通透性增加 - 可能会将这些酶释放到循环和腹膜腔中,在那里它们可能反过来激活其他酶,例如基质金属蛋白酶(MMPs)。如果不受控制,这些酶可能导致受体或血浆蛋白的病理切割。我们的第一个目标是确定在肠道外的隔室(血浆、腹膜液、脑、心脏、肝脏和肺)中蛋白酶活性,并确定失血性休克后(2 小时缺血,2 小时再灌注)的选择蛋白酶浓度。我们的第二个目标是确定用丝氨酸蛋白酶抑制剂(ANGD)抑制肠腔中的蛋白酶是否会减少远离肠道的蛋白酶活性。为了确定蛋白酶活性,将血浆和腹膜液与小肽底物孵育,用于胰蛋白酶、糜蛋白酶和弹性蛋白酶样活性,或与被多种蛋白酶切割的酪蛋白孵育。明胶酶活性通过明胶凝胶酶谱法和特定的 MMP-9 底物确定。免疫印迹用于确认失血性休克后血浆、腹膜液和肺中升高的胰蛋白酶和所有样本中的 MMP-9 浓度。无论肠内预先用 ANGD 治疗,失血性休克后所有样品中的酪蛋白水解、胰蛋白酶、糜蛋白酶、弹性蛋白酶样和 MMP-9 活性均显著(p<0.05)上调。失血性休克后在血浆、腹膜空间和肺中通过免疫印迹检测到胰蛋白酶。失血性休克后,血浆、腹膜液、心脏、肝脏和肺中的 MMP-9 浓度和活性均显著上调。这些结果表明,失血性休克后,包括胰蛋白酶在内的蛋白酶活性在远离肠道的部位增加。蛋白酶,包括胰蛋白酶,可能是休克介质,也是休克治疗的潜在靶点。