Westreich Daniel, Evans Denise, Firnhaber Cindy, Majuba Pappie, Maskew Mhairi
Department of Obstetrics and Gynecology and Duke Global Health Institute, Duke University, Durham, NC 27710, USA.
J Acquir Immune Defic Syndr. 2012 Aug 15;60(5):489-94. doi: 10.1097/QAI.0b013e318256b310.
Pregnancy is a common indication for initiation of highly active antiretroviral therapy (HAART) in sub-Saharan Africa. Our objective was to evaluate how pregnancy at treatment initiation predicts virologic response to HAART.
We evaluated an open cohort of 9173 patients who initiated HAART between April 2004 and September 2009 in the Themba Lethu Clinic in Johannesburg, South Africa. Risk ratios were estimated using log-binomial regression; hazard ratios were estimated using Cox proportional hazards models; time ratios were estimated using accelerated failure time models. We controlled for calendar date, age, ethnicity, employment status, history of smoking, tuberculosis, WHO stage, weight, body mass index, hemoglobin, CD4 count and CD4 percent, and whether clinical care was free. Extensive sensitivity and secondary analyses were performed.
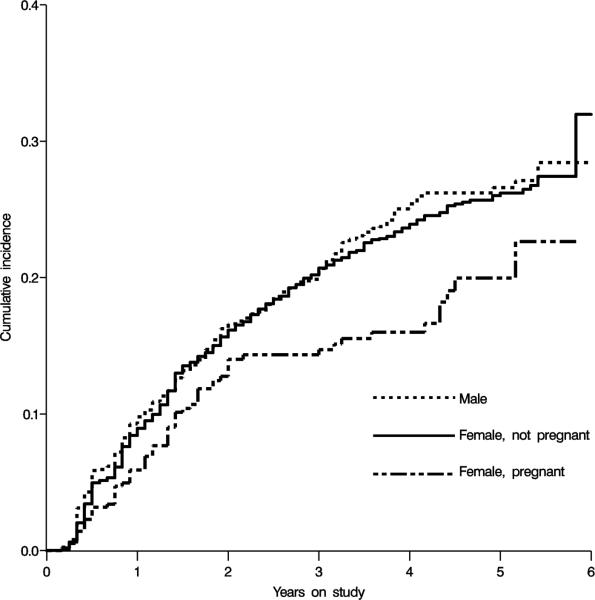
During follow-up, 822 nonpregnant women and 70 pregnant women experienced virologic failure. In adjusted analyses, pregnancy at baseline was associated with reduced risk of virologic failure by 6 months [risk ratio 0.66, 95% confidence limits (CL): 0.35 to 1.22] and with reduced hazard of virologic failure over follow-up (hazard ratio: 0.69, 95% CL: 0.50 to 0.95). The adjusted time ratio for failure was 1.44 (95% CL: 1.13 to 1.84), indicating 44% longer time to event among women pregnant at baseline. Sensitivity analyses generally confirmed main findings.
Pregnancy at HAART initiation is not associated with increased risk of virologic failure at 6 months or during longer follow-up.
在撒哈拉以南非洲地区,怀孕是开始高效抗逆转录病毒治疗(HAART)的常见指征。我们的目的是评估治疗开始时怀孕对HAART病毒学反应的预测情况。
我们评估了一个开放队列,该队列由9173例于2004年4月至2009年9月在南非约翰内斯堡的Themba Lethu诊所开始接受HAART治疗的患者组成。风险比采用对数二项回归估计;风险比采用Cox比例风险模型估计;时间比采用加速失效时间模型估计。我们对日历日期、年龄、种族、就业状况、吸烟史、结核病、世界卫生组织分期、体重、体重指数、血红蛋白、CD4细胞计数和CD4百分比,以及临床护理是否免费进行了控制。进行了广泛的敏感性分析和二次分析。
在随访期间,822名未怀孕女性和70名怀孕女性出现病毒学失败。在调整分析中,基线时怀孕与6个月时病毒学失败风险降低相关[风险比0.66,95%置信区间(CL):0.35至1.22],且与随访期间病毒学失败风险降低相关(风险比:0.69,95%CL:0.50至0.95)。失败的调整时间比为1.44(95%CL:1.13至1.84),表明基线时怀孕的女性发生事件的时间长44%。敏感性分析总体上证实了主要发现。
开始HAART治疗时怀孕与6个月时或更长随访期间病毒学失败风险增加无关。