Onoya Dorina, Sineke Tembeka, Brennan Alana T, Long Lawrence, Fox Matthew P
aHealth Economics and Epidemiology Research Office, Department of Internal Medicine, School of Clinical Medicine, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa bDepartment of Global Health cDepartment of Epidemiology, Boston University School of Public Health, Boston, Massachusetts, USA.
AIDS. 2017 Jul 17;31(11):1593-1602. doi: 10.1097/QAD.0000000000001517.
We assessed the association between the timing of pregnancy with the risk of postpartum virologic failure and loss from HIV care in South Africa.
This is a retrospective cohort study of 6306 HIV-positive women aged 15-49 at antiretroviral therapy (ART) initiation, initiated on ART between January 2004 and December 2013 in Johannesburg, South Africa.
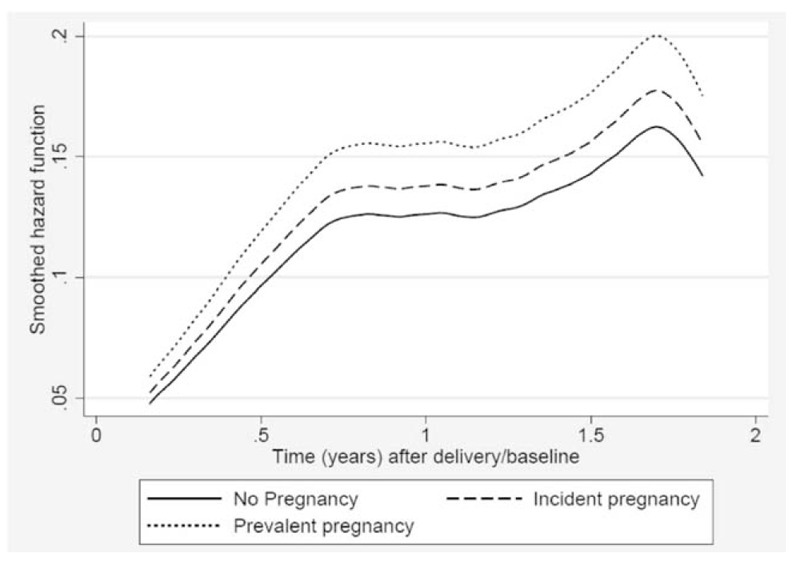
The incidence of virologic failure (two consecutive viral load measurements of >1000 copies/ml) and loss to follow-up (>3 months late for a visit) during 24 months postpartum were assessed using Cox proportional hazards modelling.
The rate of postpartum virologic failure was higher following an incident pregnancy on ART [adjusted hazard ratio 1.8, 95% confidence interval (CI): 1.1-2.7] than among women who initiated ART during pregnancy. This difference was sustained among women with CD4 cell count less than 350 cells/μl at delivery (adjusted hazard ratio 1.8, 95% CI: 1.1-3.0). Predictors of postpartum virologic failure were being viremic, longer time on ART, being 25 or less years old and low CD4 cell count and anaemia at delivery, as well as initiating ART on stavudine-containing or abacavir-containing regimen. There was no difference postpartum loss to follow-up rates between the incident pregnancies group (hazard ratio 0.9, 95% CI: 0.7-1.1) and those who initiated ART in pregnancy.
The risk of virologic failure remains high among postpartum women, particularly those who conceive on ART. The results highlight the need to provide adequate support for HIV-positive women with fertility intention after ART initiation and to strengthen monitoring and retention efforts for postpartum women to sustain the benefits of ART.
我们评估了南非妊娠时机与产后病毒学失败风险及HIV治疗失访之间的关联。
这是一项回顾性队列研究,研究对象为2004年1月至2013年12月在南非约翰内斯堡开始接受抗逆转录病毒治疗(ART)的6306名年龄在15 - 49岁的HIV阳性女性。
使用Cox比例风险模型评估产后24个月内病毒学失败(连续两次病毒载量测量>1000拷贝/ml)和失访(就诊延迟>3个月)的发生率。
与孕期开始接受ART的女性相比,ART期间意外怀孕后的产后病毒学失败率更高[调整后风险比1.8,95%置信区间(CI):1.1 - 2.7]。这种差异在分娩时CD4细胞计数低于350个/μl的女性中持续存在(调整后风险比1.8,95% CI:1.1 - 3.0)。产后病毒学失败的预测因素包括病毒血症、ART治疗时间较长、年龄在25岁及以下、分娩时CD4细胞计数低和贫血,以及开始使用含司他夫定或含阿巴卡韦的治疗方案。意外怀孕组与孕期开始接受ART的组之间产后失访率没有差异(风险比0.9,95% CI:0.7 - 1.1)。
产后女性,尤其是那些在ART期间怀孕的女性,病毒学失败的风险仍然很高。结果强调需要为ART开始后有生育意愿的HIV阳性女性提供充分支持,并加强对产后女性的监测和留存工作,以维持ART的益处。