Department of Population Health and Primary Care, Norwich Medical School, University of East Anglia, Norwich, UK.
BMC Health Serv Res. 2012 Apr 16;12:94. doi: 10.1186/1472-6963-12-94.
The General Medical Services primary care contract for the United Kingdom financially rewards performance in 19 clinical areas, through the Quality and Outcomes Framework. Little is known about how best to determine the size of financial incentives in pay for performance schemes. Our aim was to test the hypothesis that performance indicators with larger population health benefits receive larger financial incentives.
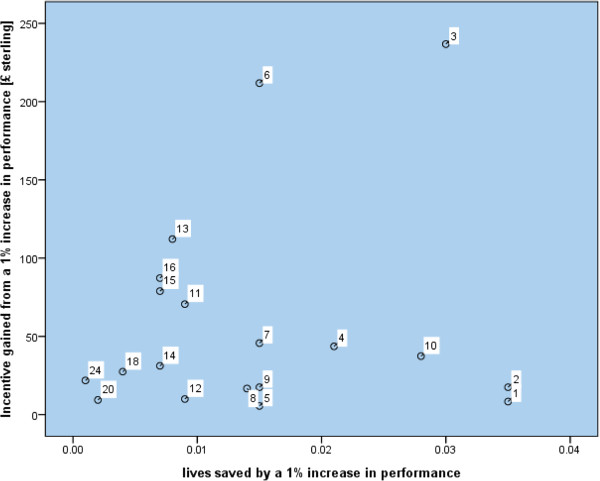
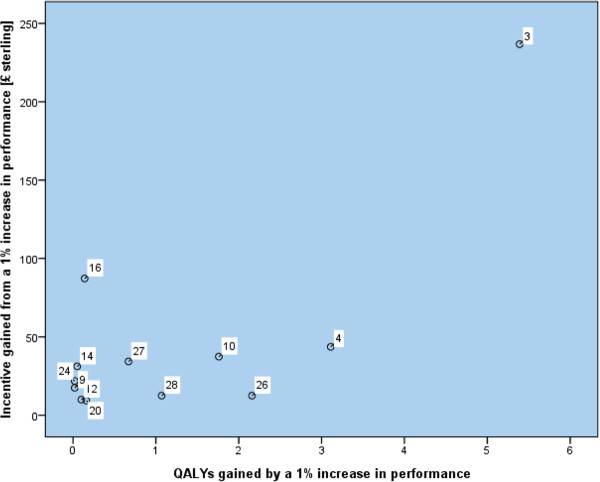
We performed cross sectional analyses to quantify associations between the size of financial incentives and expected health gain in the 2004 and 2006 versions of the Quality and Outcomes Framework. We used non-parametric two-sided Spearman rank correlation tests. Health gain was measured in expected lives saved in one year and in quality adjusted life years. For each quality indicator in an average sized general practice we tested for associations first, between the marginal increase in payment and the health gain resulting from a one percent point improvement in performance and second, between total payment and the health gain at the performance threshold for maximum payment.
Evidence for lives saved or quality adjusted life years gained was found for 28 indicators accounting for 41% of the total incentive payments. No statistically significant associations were found between the expected health gain and incentive gained from a marginal 1% increase in performance in either the 2004 or 2006 version of the Quality and Outcomes Framework. In addition no associations were found between the size of financial payment for achievement of an indicator and the expected health gain at the performance threshold for maximum payment measured in lives saved or quality adjusted life years.
In this subgroup of indicators the financial incentives were not aligned to maximise health gain. This disconnection between incentive and expected health gain risks supporting clinical activities that are only marginally effective, at the expense of more effective activities receiving lower incentives. When designing pay for performance programmes decisions about the size of the financial incentive attached to an indicator should be informed by information on the health gain to be expected from that indicator.
英国的全科医疗服务合同通过质量和结果框架,在 19 个临床领域对绩效进行经济奖励。对于如何确定绩效薪酬方案中的经济激励规模,知之甚少。我们的目的是检验这样一个假设,即对人群健康有较大益处的绩效指标会得到更大的经济激励。
我们进行了横断面分析,以量化 2004 年和 2006 年质量和结果框架中经济激励的规模与预期健康收益之间的关联。我们使用非参数双边 Spearman 秩相关检验。健康收益以预期一年内节省的生命和质量调整生命年来衡量。对于每个普通规模的一般实践中的质量指标,我们首先测试了支付的边际增量与因绩效提高 1 个百分点而导致的健康收益之间的关联,其次测试了总支付与最大支付绩效阈值的健康收益之间的关联。
有 28 个指标(占总激励支付的 41%)存在与节省生命或质量调整生命年相关的证据。在 2004 年或 2006 年质量和结果框架的任何一个版本中,都没有发现边际绩效提高 1%所带来的预期健康收益与激励收益之间存在统计学显著关联。此外,在达到指标的绩效阈值时,实现指标的财务支付规模与最大支付绩效阈值的预期健康收益之间也没有关联,以节省生命或质量调整生命年来衡量。
在这一组指标中,经济激励并未与最大化健康收益保持一致。激励与预期健康收益之间的这种脱节,可能会支持那些效果只是略有改善的临床活动,而牺牲了更有效的活动获得较低的激励。在设计绩效薪酬方案时,应根据从该指标获得的预期健康收益信息来决定与指标相关的经济激励规模。