Ang Marcus, Cheung Gemmy, Vania Maya, Chen Jinmiao, Yang Henry, Li Jing, Chee Soon-Phaik
Singapore National Eye Centre, Singapore.
Mol Vis. 2012;18:565-73. Epub 2012 Mar 2.
The aim of this study was to study the aqueous cytokine and chemokine composition in patients with uveitis associated with tuberculosis (TAU).
We present a prospective case series of consecutive new patients with active uveitis presenting at a single tertiary center (January 1, 2008-January 1, 2010). Patients with no ocular pathology other than cataracts were enrolled as non-inflammatory controls. Aqueous samples were taken from all study subjects and analyzed using a magnetic color-bead-based multiplex assay for cytokine and chemokine concentrations.
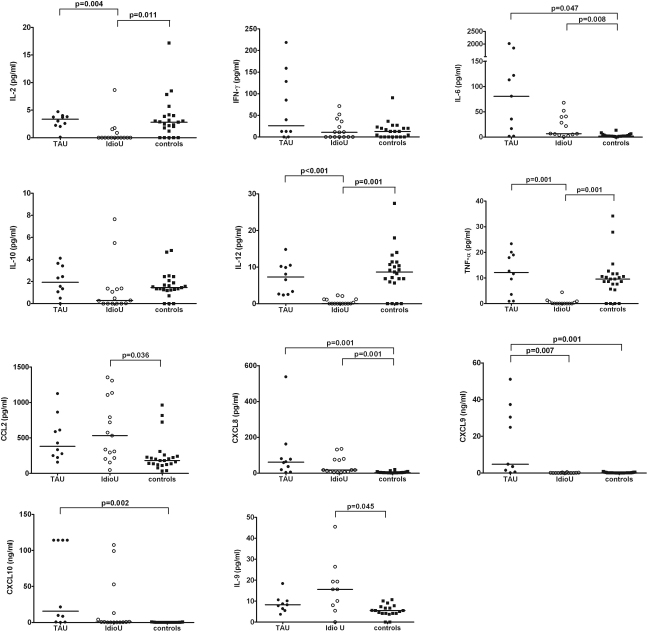
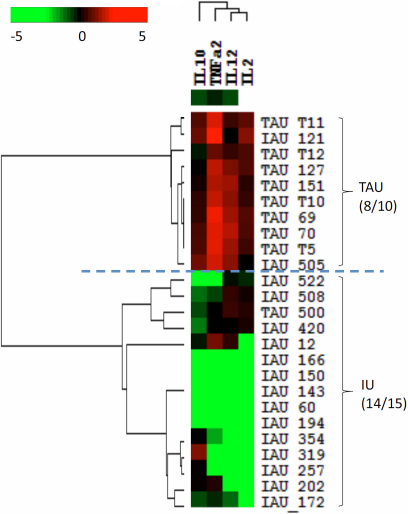
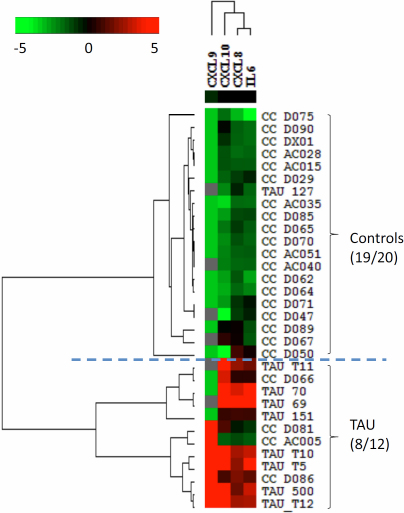
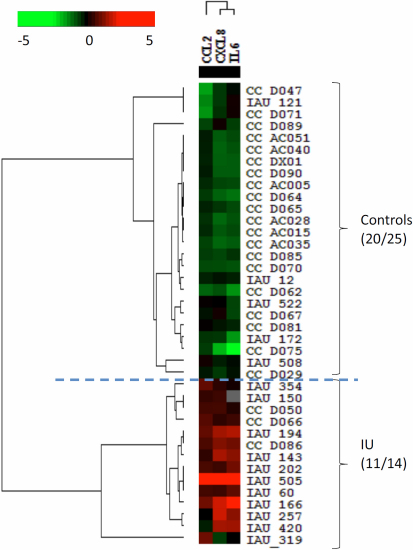
Twenty-five eyes of 25 patients with active uveitis with suspected tuberculosis (TB) and 23 non-inflammatory controls were enrolled. Ten patients tested positive on a tuberculin skin test and interferon-gamma release assay; all ten patients responded to anti-TB treatment with no recurrences (TAU). The remaining 15 eyes were negative for the above tests and had no other underlying causes for uveitis found on clinical evaluation and investigations; therefore, they were classified as "idiopathic uveitis" (IU). The TAU group showed significantly higher levels of interleukin-6 (IL-6; p=0.047), interleukin-8 (CXCL8; p=0.001), monokine induced by interferon-gamma (CXCL9; p=0.001), and interferon-gamma-induced protein 10 (IP-10 or CXCL10; p=0.002), compared to the controls. The IU group showed significantly higher levels of IL-6 (p=0.008), monocyte chemotactic protein-1 (CCL2; p=0.036), CXCL8 (p=0.001), and IL-9 (p=0.045), and significantly lower levels of IL-2 (p=0.011), IL-12 (p=0.001), and tumor necrosis factor (TNF)-α (p=0.001), compared to the controls. Heat map analysis revealed significant differences in aqueous cytokine and chemokine concentrations among the TAU patients, the IU patients, and the controls.
In our study population, aqueous cytokine and chemokine analyses suggest that subjects with uveitis associated with TB who respond to anti-TB therapy do not have an active ocular tuberculous infection, but rather an autoimmune-related ocular inflammation that may be triggered by TB.
本研究旨在探讨结核相关性葡萄膜炎(TAU)患者房水中细胞因子和趋化因子的组成。
我们呈现了一个前瞻性病例系列,纳入了在单一三级中心就诊的连续新发活动性葡萄膜炎患者(2008年1月1日至2010年1月1日)。除白内障外无其他眼部病变的患者作为非炎症对照组。采集所有研究对象的房水样本,采用基于磁珠的多重检测法分析细胞因子和趋化因子浓度。
纳入了25例疑似结核(TB)的活动性葡萄膜炎患者的25只眼和23例非炎症对照组。10例患者结核菌素皮肤试验和干扰素-γ释放试验呈阳性;所有10例患者接受抗结核治疗后均无复发(TAU)。其余15只眼上述检查为阴性,临床评估和检查未发现其他葡萄膜炎的潜在病因;因此,它们被归类为“特发性葡萄膜炎”(IU)。与对照组相比,TAU组白细胞介素-6(IL-6;p = 0.047)、白细胞介素-8(CXCL8;p = 0.001)、干扰素-γ诱导的单核因子(CXCL9;p = 0.001)和干扰素-γ诱导蛋白10(IP-10或CXCL10;p = 0.002)水平显著更高。与对照组相比,IU组IL-6(p = 0.008)、单核细胞趋化蛋白-1(CCL2;p = 0.036)、CXCL8(p = 0.001)和IL-9(p = 0.045)水平显著更高,而IL-2(p = 0.011)、IL-12(p = 0.001)和肿瘤坏死因子(TNF)-α(p = 0.001)水平显著更低。热图分析显示TAU患者、IU患者和对照组之间房水细胞因子和趋化因子浓度存在显著差异。
在我们的研究人群中,房水细胞因子和趋化因子分析表明,对抗结核治疗有反应的结核相关性葡萄膜炎患者没有活动性眼部结核感染,而是可能由结核引发的自身免疫相关眼部炎症。