Department of Radiation Oncology, Mayo Clinic, Rochester, MN, USA.
Radiat Oncol. 2012 May 3;7:67. doi: 10.1186/1748-717X-7-67.
To report single-institutional clinical outcomes and toxicity with SBRT for cholangiocarcinoma.
From March 2009 to July 2011, 10 patients with 12 unresectable primary (n = 6) or recurrent (n = 6) cholangiocarcinoma lesions underwent abdominal SBRT. Sites treated included liver (n = 10), abdominal lymph nodes (n = 1), and adrenal gland (n = 1). SBRT was delivered in three (n = 2) or five (n = 10) consecutive daily fractions over one week. The median prescription dose was 55 Gy (range, 45-60). Treatment response was graded by RECIST v.1.1, and toxicities were scored by CTCAE v.4.0. Data was analyzed using the Kaplan-Meier method to determine rates of local control (LC), freedom from distant progression (FFDM) and overall survival (OS).
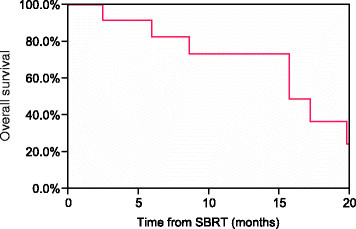
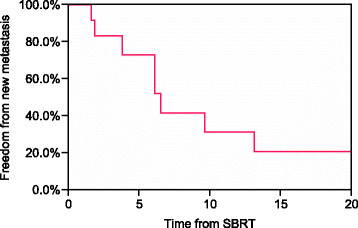
The median follow-up was 14 months (range, 2-26 months). LC, defined as freedom from progression within the SBRT field, was 100%, but four patients treated to intrahepatic sites experienced progression elsewhere in the liver. Estimates for FFDM at 6 and 12 months were 73% and 31%, respectively. Sites of disease relapse included liver (n = 3), liver and lymph nodes (n = 1), liver and lungs (n = 1), lymph nodes (n = 1), and mesentery (n = 1). OS estimates for the cohort at 6 and 12 months were 83% and 73%, respectively. The most common Grade ≥ 2 early toxicities were Grade 2 nausea and vomiting (n = 5) and gastrointestinal pain (n = 2). Late ≥ 2 toxicities included Grade 2 gastrointestinal pain (n = 3), Grade 3 biliary stenosis (n = 1), and Grade 5 liver failure (n = 1).
SBRT shows promise as an effective local therapy for properly-selected patients with cholangiocarcinoma. Further follow-up is needed to better quantify the risk of late complications associated with SBRT.
报告胆管癌立体定向体部放疗(SBRT)的单机构临床结果和毒性。
从 2009 年 3 月至 2011 年 7 月,10 例 12 处不可切除的原发性(n = 6)或复发性(n = 6)胆管癌病变患者接受了腹部 SBRT。治疗部位包括肝脏(n = 10)、腹部淋巴结(n = 1)和肾上腺(n = 1)。SBRT 在一周内分 3 次(n = 2)或 5 次(n = 10)连续每日分次进行。中位处方剂量为 55 Gy(范围 45-60)。采用 RECIST v.1.1 对治疗反应进行分级,采用 CTCAE v.4.0 对毒性进行评分。采用 Kaplan-Meier 法分析数据,以确定局部控制率(LC)、无远处进展率(FFDM)和总生存率(OS)。
中位随访时间为 14 个月(范围 2-26 个月)。LC 定义为 SBRT 范围内无进展,为 100%,但 4 例肝内治疗患者在肝脏其他部位出现进展。6 个月和 12 个月时的 FFDM 估计值分别为 73%和 31%。疾病复发部位包括肝脏(n = 3)、肝脏和淋巴结(n = 1)、肝脏和肺(n = 1)、淋巴结(n = 1)和肠系膜(n = 1)。6 个月和 12 个月时的 OS 估计值分别为 83%和 73%。最常见的≥2 级早期毒性为 2 级恶心和呕吐(n = 5)和胃肠道疼痛(n = 2)。晚期≥2 级毒性包括 2 级胃肠道疼痛(n = 3)、3 级胆道狭窄(n = 1)和 5 级肝衰竭(n = 1)。
SBRT 作为一种有效的局部治疗方法,为选择合适的胆管癌患者带来了希望。需要进一步随访以更好地量化与 SBRT 相关的晚期并发症风险。