Boedeker Carsten Christof
Department of Otorhinolaryngology, Head and Neck Surgery, University of Freiburg, Germany.
GMS Curr Top Otorhinolaryngol Head Neck Surg. 2011;10:Doc03. doi: 10.3205/cto000076. Epub 2012 Apr 26.
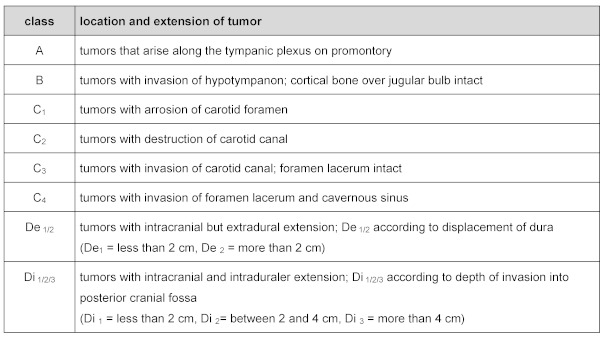
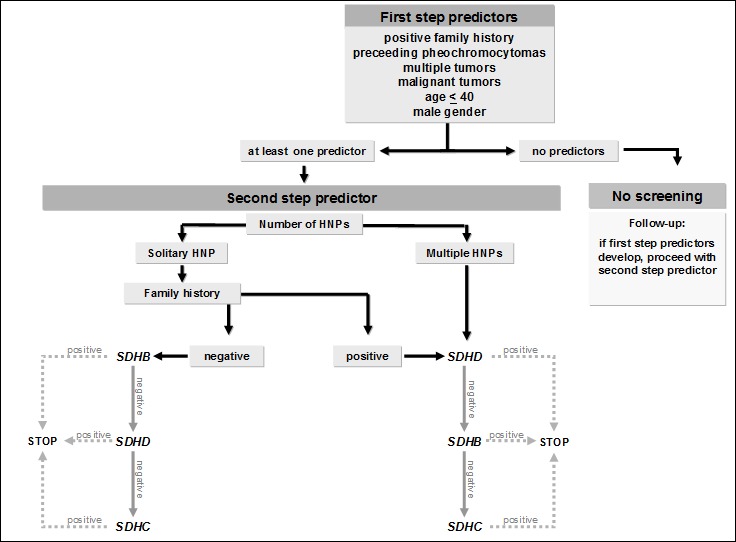
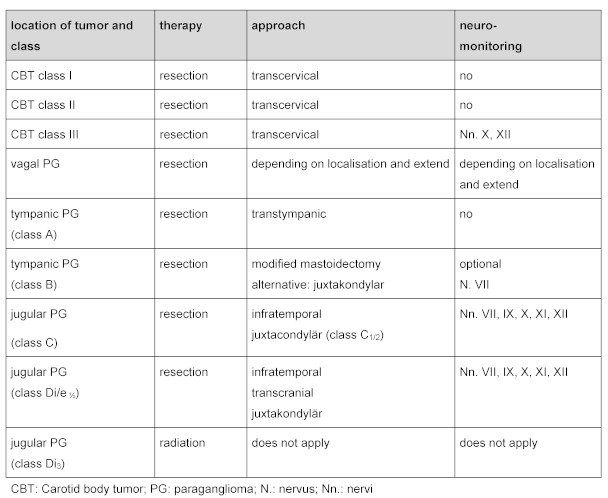
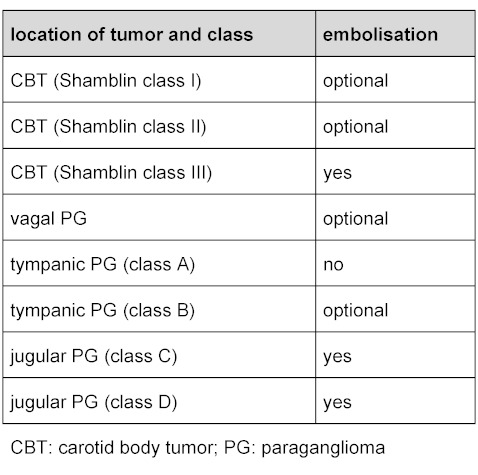
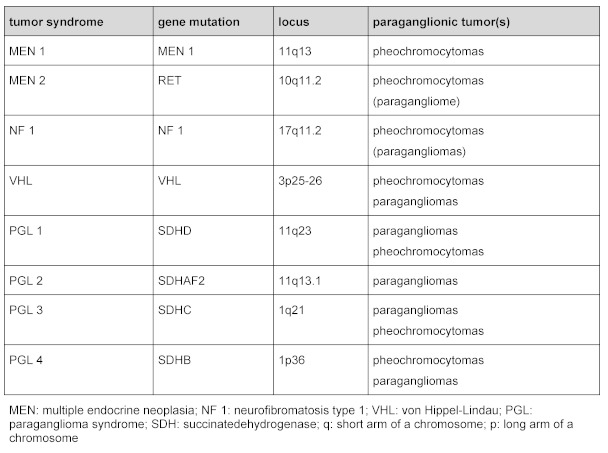
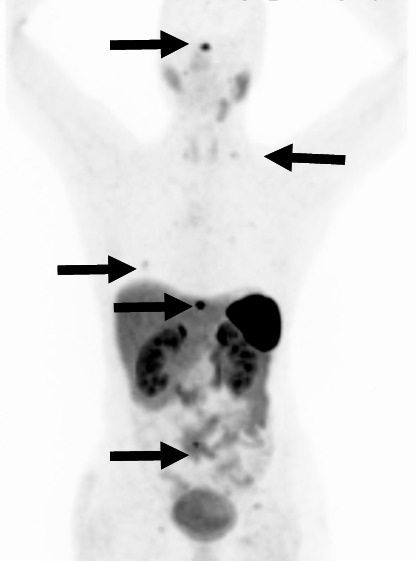
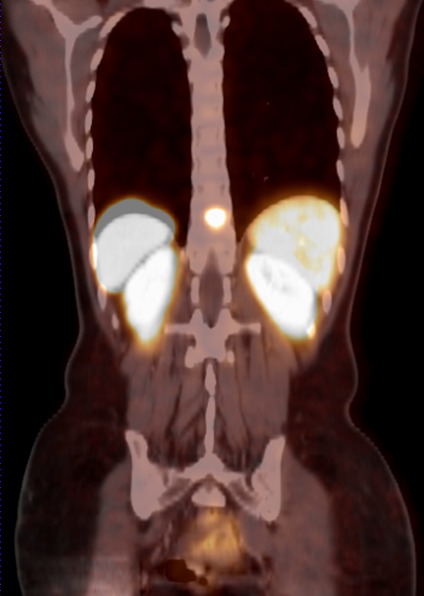
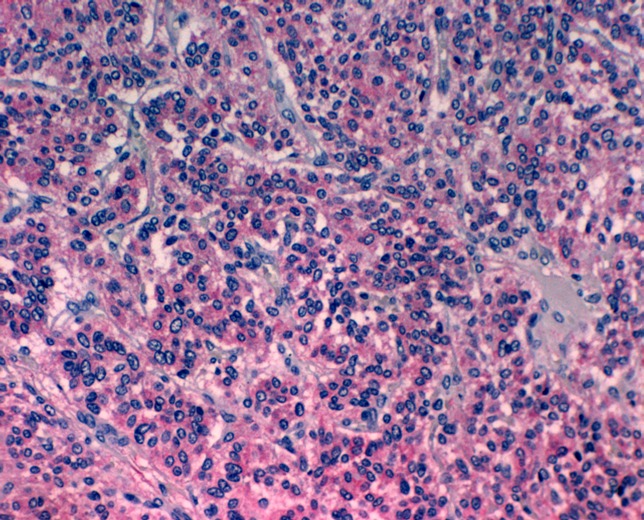
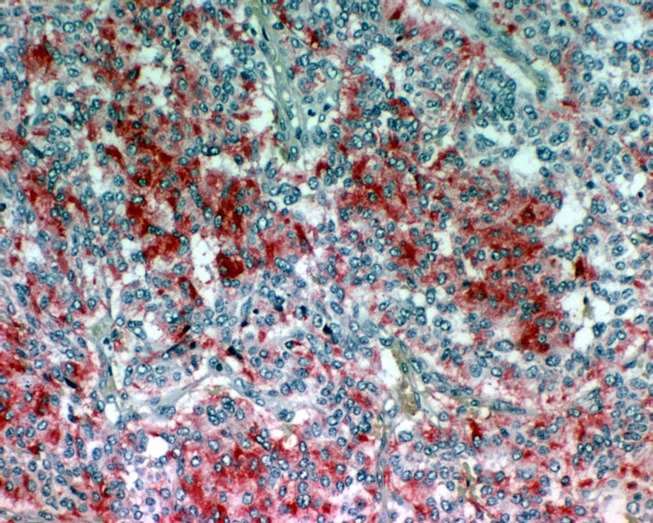
Paragangliomas are rare tumors of neural crest origin. They are benign in the majority of cases and are characterized by a strong vascularisation.In the head and neck region they most commonly occur as carotid body tumors. Jugulotympanic and especially vagal paragangliomas are seen less frequently. Complete surgical resection represents the only curative treatment option even though resection of locally advanced tumors regularly results in lesions of the lower cranial nerves and major vessels. Appoximately 30% of all head and neck paragangliomas (HNPs) are hereditary and associated with different tumor syndromes. The paraganglioma syndromes 1, 3 and 4 (PGL 1, 3 and 4) make up the majority of those familial cases. PGL 1 is associated with mutations of the succinate dehydrogenase subunit D (SDHD) gene, PGL 3 is caused by SDHC and PGL 4 by SDHB gene mutations. Multiple HNPs and the occurance of HNPs together with pheochromocytomas are seen in SDHD as well as SDHB mutation carriers. In patients with SDHB mutations the risk for the development of malignant paraganglial tumors is significantly higher compared to SDHC and SDHD patients as well as patients with sporadic tumors. SDHC mutation carriers almost exclusively present with benign HNP that are unifocal in the majority of cases. The role of transmission is autosomal dominant for all three symptoms. Interestingly, there is a "parent-of-origin-dependent-inheritance" in subjects with SDHD gene mutations. This means that the disease phenotype may only become present if the mutation is inherited through the paternal line. We recommend screening for mutations of the genes SDHB, SDHC and SDHD in patients with HNPs. Certain clinical parameters can help to set up the order in which the three genes should be tested.
副神经节瘤是起源于神经嵴的罕见肿瘤。大多数情况下为良性,其特点是血管丰富。在头颈部区域,它们最常表现为颈动脉体瘤。颈静脉鼓室副神经节瘤,尤其是迷走神经副神经节瘤较少见。完整的手术切除是唯一的治愈性治疗选择,尽管局部晚期肿瘤的切除常导致下颅神经和大血管损伤。所有头颈部副神经节瘤(HNP)中约30%为遗传性,与不同的肿瘤综合征相关。副神经节瘤综合征1、3和4(PGL 1、3和4)构成了这些家族性病例的大多数。PGL 1与琥珀酸脱氢酶亚基D(SDHD)基因突变有关,PGL 3由SDHC引起,PGL 4由SDHB基因突变引起。在SDHD以及SDHB突变携带者中可见多发HNP和HNP与嗜铬细胞瘤同时出现的情况。与SDHC和SDHD患者以及散发性肿瘤患者相比, SDHB突变患者发生恶性副神经节瘤的风险明显更高。SDHC突变携带者几乎仅表现为良性HNP,大多数情况下为单灶性。所有这三种综合征的遗传方式均为常染色体显性遗传。有趣的是,SDHD基因突变的个体存在“亲本来源依赖性遗传”。这意味着只有当突变通过父系遗传时,疾病表型才可能出现。我们建议对HNP患者进行SDHB、SDHC和SDHD基因的突变筛查。某些临床参数有助于确定这三个基因的检测顺序。