National School for Primary Care Research and UK Centre for Tobacco Control Studies, Division of Primary Care, University of Nottingham, Medical School, Queen's Medical Centre, Nottingham, NG7 2UH, England.
BMC Public Health. 2012 Jul 10;12:329. doi: 10.1186/1471-2458-12-329.
Smoking is a UK public health threat but GPs can be effective in helping patients to quit; consequently, the Quality and Outcomes Framework (QOF) incentivises the recording of smoking status and delivery of cessation advice in patients' medical records. This study investigates the association between smoking-related QOF targets and such recording, and the factors which influence these clinical activities.
For 2000 to 2008, using medical records in The Health Improvement Network (THIN) database, the annual proportions of i) patients who had a record of smoking status made in the previous 27 months and ii) current smokers recorded as receiving cessation advice in the previous 15 months were calculated. Then, for all patients at selected points before and after the QOF's implementation, data on gender, age, Townsend score, and smoking-related morbidity were extracted. Multivariate logistic regression was used to investigate individual-level characteristics associated with the recording of smoking status and cessation advice.
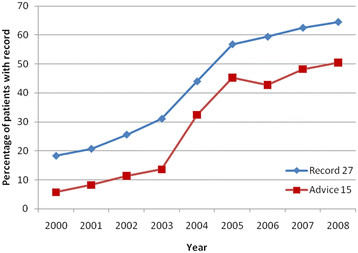
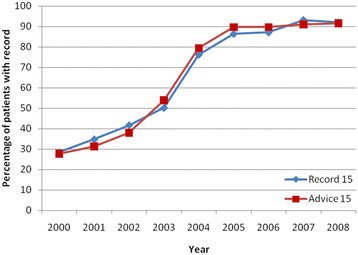
Rapid increases in recording smoking status and advice occurred around the QOF's introduction in April 2004. Subsequently, compliance to targets has been sustained, although rates of increase have slowed. By 2008 64.5% of patients aged 15+ had smoking status documented in the previous 27 months and 50.5% of current smokers had cessation advice recorded in the last 15 months. Adjusted odds ratios show that, both before and after the introduction of the QOF, those with chronic medical conditions, greater social deprivation and women were more likely to have a recent recording of smoking status or cessation advice. Since the QOF's introduction, the strongest characteristic associated with recording activities was the presence of co-morbidity. An example of this was patients with COPD, who in 2008, were 15.38 (95% CI 13.70-17.27) times and 11.72 (95% CI 10.41-13.21) times more likely to have a record of smoking status and cessation advice, respectively.
Rates of recording smoking status and cessation advice plateaued after large increases during the QOF's introduction; however, recording remains most strongly associated with the presence of chronic disease as specified by the QOF, and suggests that incentivised targets have a direct effect on clinical behaviour.
吸烟是英国公共卫生的威胁,但全科医生在帮助患者戒烟方面非常有效;因此,质量和结果框架(QOF)鼓励在患者的病历中记录吸烟状况并提供戒烟建议。本研究调查了与吸烟相关的 QOF 目标与这些记录之间的关联,以及影响这些临床活动的因素。
使用 The Health Improvement Network (THIN) 数据库中的医疗记录,对 2000 年至 2008 年期间每年记录 i)过去 27 个月内有吸烟状况记录的患者比例和 ii)过去 15 个月内有记录的当前吸烟者接受戒烟建议的比例。然后,在 QOF 实施前后的选定时间点,提取患者的性别、年龄、汤森得分和与吸烟有关的发病情况数据。使用多变量逻辑回归调查与吸烟状况和戒烟建议记录相关的个体特征。
在 2004 年 4 月 QOF 引入前后,记录吸烟状况和建议的比例迅速增加。此后,尽管增长率有所放缓,但目标的遵守情况一直保持不变。到 2008 年,64.5%的 15 岁以上患者在过去 27 个月内有吸烟状况记录,50.5%的当前吸烟者在过去 15 个月内有戒烟建议记录。调整后的优势比表明,在 QOF 引入前后,患有慢性疾病、社会贫困程度较高和女性的患者更有可能最近记录吸烟状况或戒烟建议。自 QOF 引入以来,与记录活动最相关的特征是合并症的存在。例如,2008 年 COPD 患者记录吸烟状况和戒烟建议的可能性分别是未患 COPD 患者的 15.38(95%置信区间 13.70-17.27)倍和 11.72(95%置信区间 10.41-13.21)倍。
在 QOF 引入期间大幅增加后,记录吸烟状况和戒烟建议的比例趋于平稳;然而,记录与 QOF 规定的慢性疾病的存在最密切相关,这表明激励性目标对临床行为有直接影响。