Neyt Mattias, Van Brabandt Hans, Devriese Stephan, Van De Sande Stefaan
Belgian Health Care Knowledge Centre (KCE), Brussels, Belgium.
BMJ Open. 2012 May 4;2(3). doi: 10.1136/bmjopen-2012-001032. Print 2012.
Patients with severe aortic stenosis and coexisting non-cardiac conditions may be at high risk for surgical replacement of the aortic valve or even be no candidates for surgery. In these patients, transcatheter aortic valve implantation (TAVI) is suggested as an alternative. Results of the PARTNER (Placement of AoRTic TraNscathetER Valve) trial comparing the clinical effectiveness of TAVI with surgical valve replacement and standard therapy were published. The authors assessed the cost-effectiveness of TAVI in Belgium.
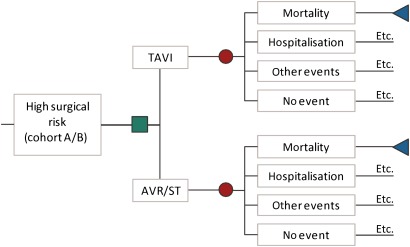
A Markov model of incremental costs, effects (survival and quality of life) and incremental cost-effectiveness of TAVI was developed. The impact on survival, number of events and quality of life was based on the PARTNER trial. Costs per event were context specific.
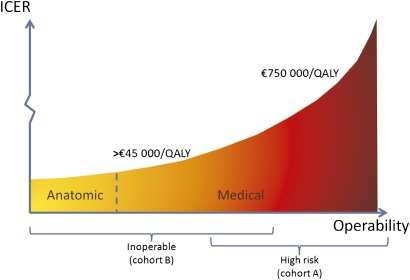
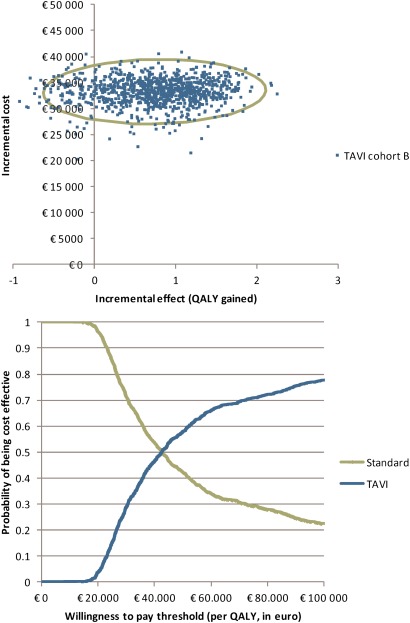
In high-risk operable patients, even if the minor differences in 30-day and 1-year mortality are taken into account, the incremental cost-effectiveness ratio (ICER) remains on average above €750 000 per quality-adjusted life-year (QALY) gained (incremental cost: €20 400; incremental effect: 0.03 QALYs). In inoperable patients, an ICER of €44 900 per QALY (incremental cost: €33 200; incremental effect: 0.74 QALYs) is calculated, including a life-long extrapolation of the mortality benefit. This result was sensitive to the assumed time horizon. The subgroup of anatomically inoperable patients had better outcomes than medically inoperable patients, with ICERs decreasing more than €10 000/QALY.
It is inappropriate to consider reimbursement of TAVI for high-risk operable patients. Reimbursing TAVI in inoperable patients in essence is a political decision. From an economic perspective, it would be prudent to first target patients that are inoperable because of anatomical prohibitive conditions. In the search for evidence, the authors identified non-published negative results from a randomised controlled TAVI trial. The study sponsor should be more willing to share this information to allow balanced evaluations and policy recommendations. Payers should require these data before taking reimbursement decisions.
患有严重主动脉瓣狭窄并伴有非心脏疾病的患者,进行主动脉瓣手术置换的风险可能很高,甚至可能不适合接受手术。对于这些患者,建议采用经导管主动脉瓣植入术(TAVI)作为替代方案。比较TAVI与外科瓣膜置换及标准治疗的临床疗效的PARTNER(经导管主动脉瓣置入)试验结果已发表。作者评估了TAVI在比利时的成本效益。
建立了一个关于TAVI的增量成本、效果(生存和生活质量)以及增量成本效益的马尔可夫模型。对生存、事件数量和生活质量的影响基于PARTNER试验。每个事件的成本因具体情况而异。
在高危可手术患者中,即使考虑到30天和1年死亡率的微小差异,每获得一个质量调整生命年(QALY)的增量成本效益比(ICER)平均仍高于750,000欧元(增量成本:20,400欧元;增量效果:0.03 QALY)。在不可手术患者中,计算得出的ICER为每QALY 44,900欧元(增量成本:33,200欧元;增量效果:0.74 QALY),包括对死亡率获益的终身外推。这一结果对假定的时间范围敏感。解剖学上不可手术的患者亚组比医学上不可手术的患者预后更好,ICER每QALY降低超过10,000欧元。
考虑为高危可手术患者报销TAVI是不合适的。为不可手术患者报销TAVI本质上是一个政治决定。从经济角度看,首先将因解剖学限制条件而不可手术的患者作为目标更为审慎。在寻找证据的过程中,作者发现了一项随机对照TAVI试验未发表的阴性结果。研究主办方应更愿意分享这些信息,以便进行全面评估和制定政策建议。支付方在做出报销决定前应要求提供这些数据。