Department of Rheumatology, Cochin Hospital, Paris, France.
Ann Rheum Dis. 2013 Jan;72(1):43-50. doi: 10.1136/annrheumdis-2011-201282. Epub 2012 May 5.
In patients with active rheumatoid arthritis (RA) despite methotrexate, to compare the efficacy of adding tocilizumab to that of switching to tocilizumab monotherapy.
Double-blind, 2-year study in which adults with active RA (DAS28 >4.4) despite methotrexate were randomly assigned either to continue methotrexate with the addition of tocilizumab (MTX+TCZ) 8 mg/kg every 4 weeks or switch to tocilizumab and placebo (TCZ+PBO). The primary endpoint was the DAS28-erythrocyte sedimentation rate (ESR) remission rate at week 24. Secondary objectives included other symptomatic outcomes, quality of life and progression of structural damage.
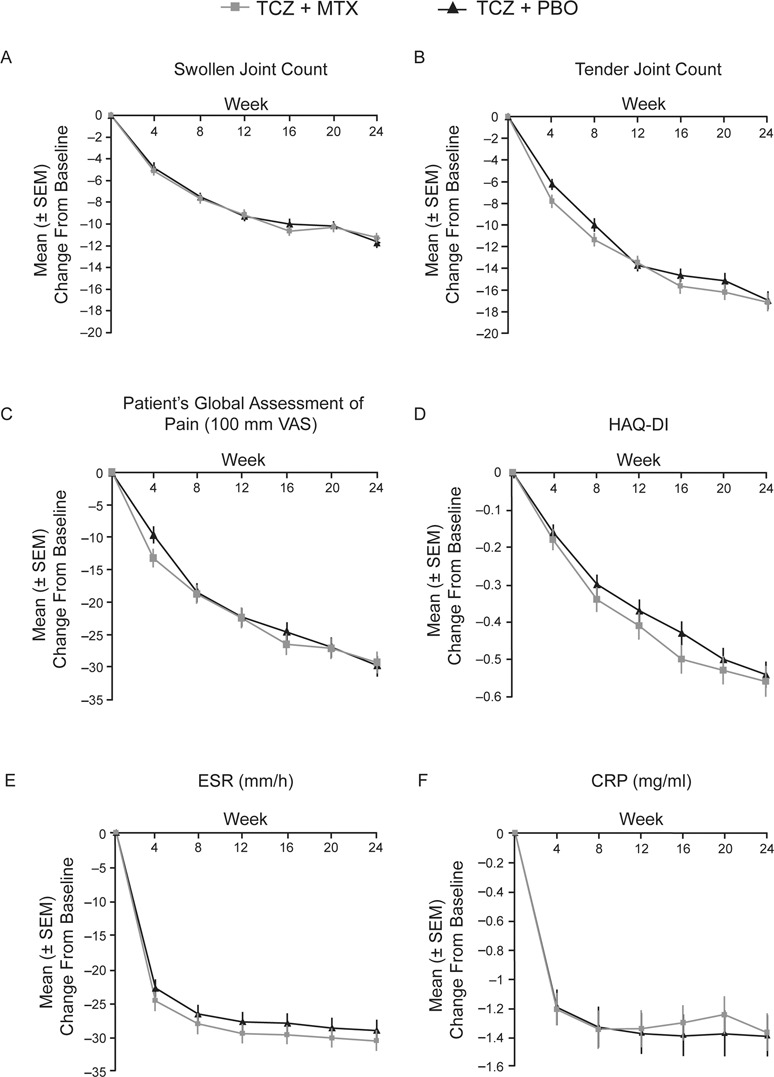
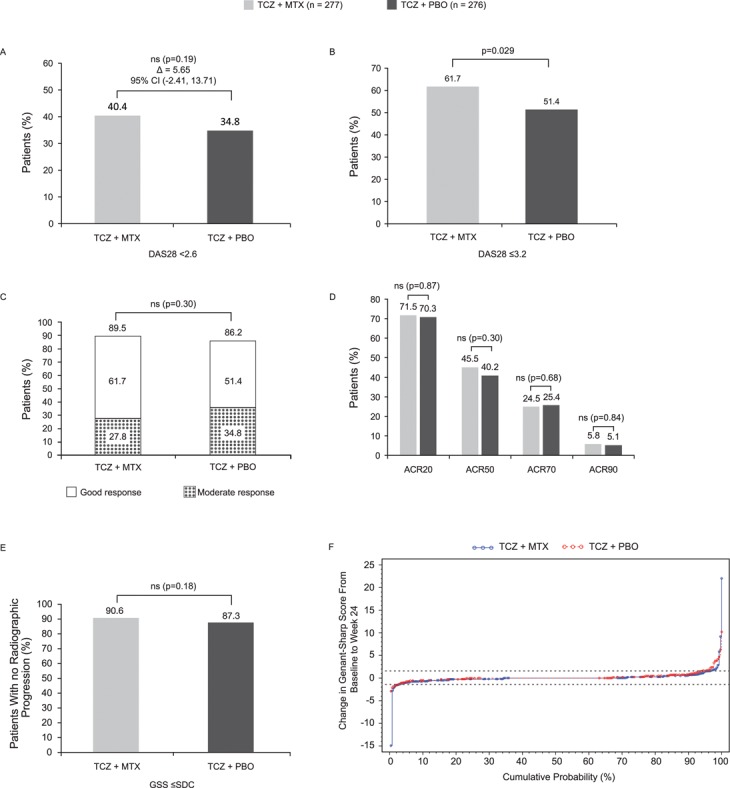
Of 556 randomly assigned patients, 512 (92%) completed 24 weeks. DAS28-ESR remission rates were 40.4% for TCZ+MTX and 34.8% for TCZ+PBO (p=0.19); American College of Rheumatology 20/50/70/90 rates were 71.5%/45.5%/24.5%/5.8% (TCZ+MTX) and 70.3%/40.2%/25.4%/5.1% (TCZ+PBO; differences not significant). A significant difference between groups was seen for low DAS28 (61.7% vs 51.4%). Radiographic progression was small and not different between groups (Genant-Sharp score progression ≤ smallest detectable change in 91% (TCZ+MTX) and 87% (TCZ+PBO)). Rates per 100 patient-years of serious adverse events and serious infections were 21 and six, respectively, for TCZ+MTX and 18 and six, respectively, for TCZ+PBO. Alanine aminotransferase elevations greater than threefold the upper limit of normal occurred in 7.8% and 1.2% of TCZ+MTX and TCZ+PBO patients, respectively.
No clinically relevant superiority of the TCZ+MTX add-on strategy over the switch to tocilizumab monotherapy strategy was observed. The combination was more commonly associated with transaminase increases. Meaningful clinical and radiographic responses were achieved with both strategies, suggesting that tocilizumab monotherapy might be a valuable treatment strategy in suitable RA patients.
在甲氨蝶呤治疗下仍处于活动期的类风湿关节炎(RA)患者中,比较添加托珠单抗与转换为托珠单抗单药治疗的疗效。
这是一项为期 2 年的双盲研究,纳入了甲氨蝶呤治疗下仍处于活动期(DAS28>4.4)的成人 RA 患者,他们被随机分为继续甲氨蝶呤联合托珠单抗 8mg/kg 每 4 周(MTX+TCZ)组或转换为托珠单抗联合安慰剂(TCZ+PBO)组。主要终点是第 24 周时 DAS28-红细胞沉降率(ESR)缓解率。次要终点包括其他症状缓解情况、生活质量和结构损伤进展。
在 556 名随机分配的患者中,有 512 名(92%)完成了 24 周的治疗。TCZ+MTX 组和 TCZ+PBO 组的 DAS28-ESR 缓解率分别为 40.4%和 34.8%(p=0.19);美国风湿病学会 20/50/70/90 缓解率分别为 71.5%/45.5%/24.5%/5.8%(TCZ+MTX)和 70.3%/40.2%/25.4%/5.1%(TCZ+PBO);差异无统计学意义。两组之间低 DAS28(61.7% vs 51.4%)的缓解率有显著差异。影像学进展较小,两组之间无差异(Genant-Sharp 评分进展≤最小可检测变化,TCZ+MTX 组为 91%,TCZ+PBO 组为 87%)。TCZ+MTX 组和 TCZ+PBO 组的每 100 患者年严重不良事件和严重感染的发生率分别为 21 例和 6 例,分别为 18 例和 6 例。TCZ+MTX 组和 TCZ+PBO 组分别有 7.8%和 1.2%的患者丙氨酸氨基转移酶升高超过正常值的 3 倍。
与转换为托珠单抗单药治疗策略相比,TCZ+MTX 联合治疗策略没有观察到具有临床意义的优越性。联合治疗更常见的是转氨酶升高。两种策略都取得了有意义的临床和影像学缓解,表明托珠单抗单药治疗可能是适合 RA 患者的一种有价值的治疗策略。