Dartmouth-Hitchcock Medical Center, Lebanon, NH, USA.
Aliment Pharmacol Ther. 2012 Jul;36(1):3-15. doi: 10.1111/j.1365-2036.2012.05128.x. Epub 2012 May 16.
Functional dyspepsia (FD), a common functional gastrointestinal disorder, is defined by the Rome III criteria as symptoms of epigastric pain or discomfort (prevalence in FD of 89-90%), postprandial fullness (75-88%), and early satiety (50-82%) within the last 3 months with symptom onset at least 6 months earlier. Patients cannot have any evidence of structural disease to explain symptoms and predominant symptoms of gastroesophageal reflux are exclusionary. Symptoms of FD are non-specific and the pathophysiology is diverse, which explains in part why a universally effective treatment for FD remains elusive.
To present current management options for the treatment of FD (therapeutic gain/response rate noted when available).
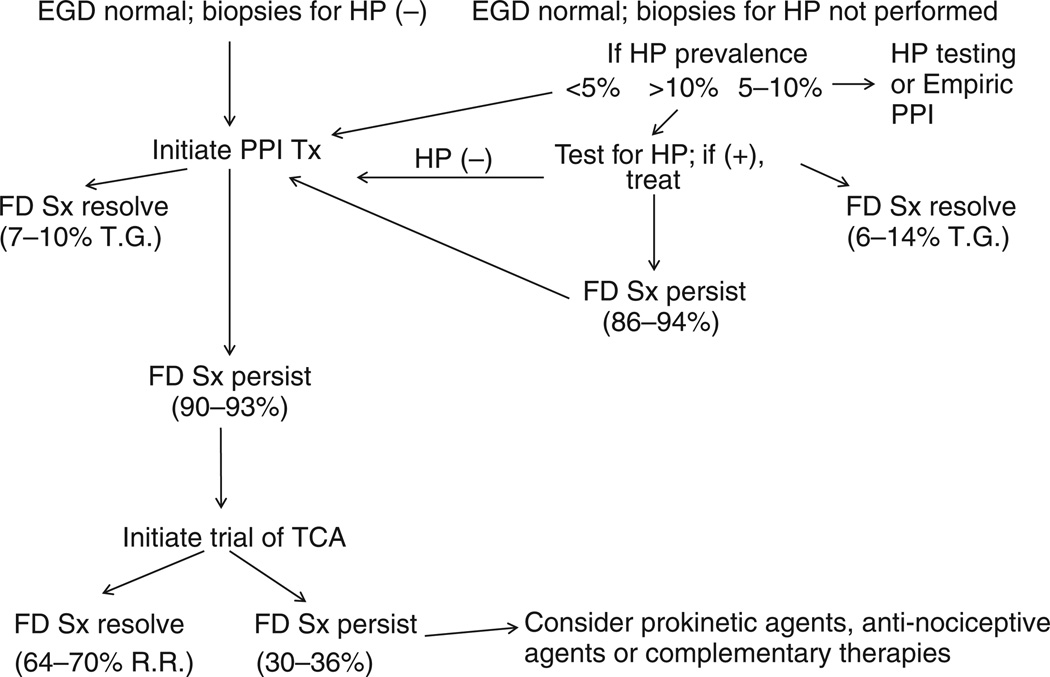
The utility of Helicobacter pylori eradication for the treatment of FD is modest (6-14% therapeutic gain), while the therapeutic efficacy of proton pump inhibitors (PPI) (7-10% therapeutic gain), histamine-type-2-receptor antagonists (8-35% therapeutic gain), prokinetic agents (18-45%), tricyclic antidepressants (TCA) (response rates of 64-70%), serotonin reuptake inhibitors (no better than placebo) is limited and hampered by inadequate data. This review discusses dietary interventions and analyses studies involving complementary and alternative medications, and psychological therapies.
A reasonable treatment approach based on current evidence is to initiate therapy with a daily PPI in H. pylori-negative FD patients. If symptoms persist, a therapeutic trial with a tricyclic antidepressant may be initiated. If symptoms continue, the clinician can possibly initiate therapy with an anti-nociceptive agent, a prokinetic agent, or some form of complementary and alternative medications, although evidence from prospective studies to support this approach is limited.
功能性消化不良(FD)是一种常见的功能性胃肠道疾病,根据罗马 III 标准定义为上腹痛或不适(FD 的患病率为 89-90%)、餐后饱胀(75-88%)和早饱(50-82%)症状,症状发作至少早于 6 个月。患者不能有任何结构疾病的证据来解释症状,而胃食管反流的主要症状是排他性的。FD 的症状是非特异性的,其病理生理学是多种多样的,这部分解释了为什么 FD 的普遍有效治疗方法仍然难以捉摸。
介绍 FD 治疗的当前管理选择(治疗效果/反应率在可用时注明)。
幽门螺杆菌根除治疗 FD 的效果有限(治疗效果增加 6-14%),而质子泵抑制剂(PPI)(治疗效果增加 7-10%)、组胺 H2 受体拮抗剂(治疗效果增加 8-35%)、促动力药物(治疗效果增加 18-45%)、三环类抗抑郁药(TCA)(反应率为 64-70%)、5-羟色胺再摄取抑制剂(不比安慰剂好)的疗效有限,且受到数据不足的限制。本综述讨论了饮食干预和涉及补充和替代药物以及心理治疗的研究分析。
根据当前证据,一种合理的治疗方法是在 H. pylori 阴性 FD 患者中开始每日使用 PPI 进行治疗。如果症状持续存在,可以开始使用三环类抗抑郁药进行治疗试验。如果症状持续存在,临床医生可能可以开始使用镇痛剂、促动力药物或某种形式的补充和替代药物进行治疗,尽管支持这种方法的前瞻性研究证据有限。