Correspondence to Marije F Bakker, UMC Utrecht, Department of Rheumatology & Clinical Immunology, Utrecht PO BOX 85500, The Netherlands.
Ann Rheum Dis. 2012 Oct;71(10):1692-7. doi: 10.1136/annrheumdis-2011-200963. Epub 2012 May 17.
To evaluate the performance of individual biomarkers and a multi-biomarker disease activity (MBDA) score in the early rheumatoid arthritis (RA) patient population from the computer assisted management in early rheumatoid arthritis (CAMERA) study.
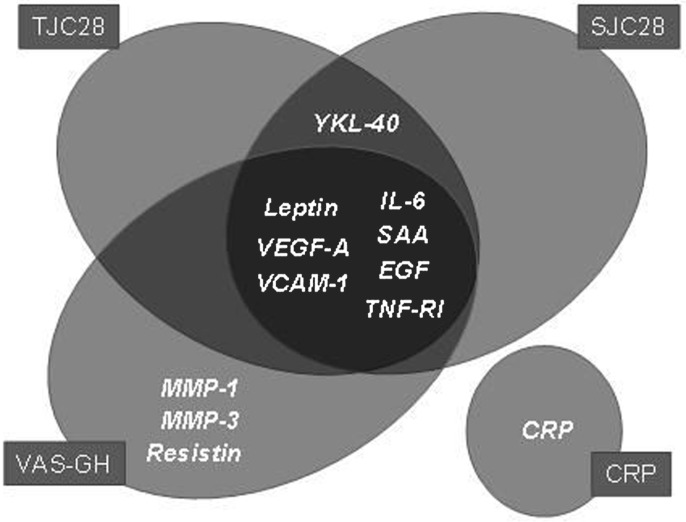
Twenty biomarkers were measured in the CAMERA cohort, in which patients were treated with either intensive or conventional methotrexate-based treatment strategies. The MBDA score was calculated using the concentrations of 12 biomarkers (SAA, IL-6, TNF-RI, VEGF-A, MMP-1, YKL-40, MMP-3, EGF, VCAM-1, leptin, resistin and CRP) according to a previously trained algorithm. The performance of the scores was evaluated relative to clinical disease activity assessments. Change in MBDA score over time was assessed by paired Wilcoxon rank sum test. Logistic regression was used to evaluate the ability of disease activity measures to predict radiographic progression.
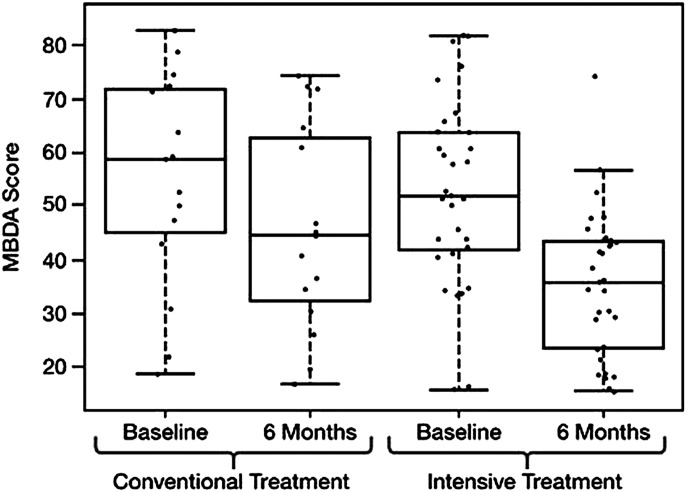
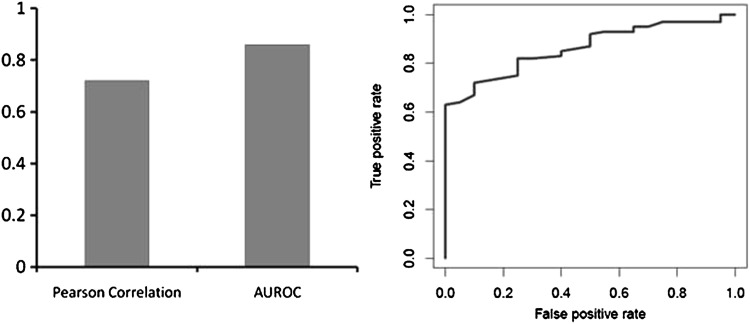
The MBDA score had a significant correlation with the disease activity score based on 28 joints-C reactive protein (DAS28-CRP) (r=0.72; p<0.001) and an area under the receiver operating characteristic curve for distinguishing remission/low from moderate/high disease activity of 0.86 (p<0.001) using a DAS28-CRP cut-off of 2.7. In multivariate analysis the MBDA score, but not CRP, was an independent predictor of disease activity measures. Additionally, mean (SD) MBDA score decreased from 53 (18) at baseline to 39 (16) at 6 months in response to study therapy (p<0.0001). Neither MBDA score nor clinical variables were predictive of radiographic progression.
This multi-biomarker test performed well in the assessment of disease activity in RA patients in the CAMERA study. Upon further validation, this test could be used to complement currently available disease activity measures and improve patient care and outcomes.
评估计算机辅助管理早期类风湿关节炎(CAMERA)研究中早期类风湿关节炎(RA)患者群体中个体生物标志物和多生物标志物疾病活动(MBDA)评分的性能。
在 CAMERA 队列中测量了 20 种生物标志物,其中患者接受了强化或常规甲氨蝶呤为基础的治疗策略。MBDA 评分根据先前训练的算法,根据 12 种生物标志物(SAA、IL-6、TNF-RI、VEGF-A、MMP-1、YKL-40、MMP-3、EGF、VCAM-1、瘦素、抵抗素和 CRP)的浓度进行计算。通过配对 Wilcoxon 秩和检验评估评分的性能与临床疾病活动评估的相关性。通过配对 Wilcoxon 秩和检验评估随时间变化的 MBDA 评分变化。逻辑回归用于评估疾病活动测量值预测放射学进展的能力。
MBDA 评分与基于 28 个关节的 C 反应蛋白(DAS28-CRP)的疾病活动评分(r=0.72;p<0.001)具有显著相关性,并且用于区分缓解/低疾病活动与中度/高疾病活动的受试者工作特征曲线下面积为 0.86(p<0.001),DAS28-CRP 截断值为 2.7。在多变量分析中,MBDA 评分,而不是 CRP,是疾病活动测量的独立预测因子。此外,MBDA 评分从基线时的 53(18)在研究治疗后降低到 6 个月时的 39(16)(p<0.0001)。MBDA 评分和临床变量均不能预测放射学进展。
本多生物标志物试验在 CAMERA 研究中评估 RA 患者的疾病活动方面表现良好。进一步验证后,该试验可用于补充目前可用的疾病活动测量方法,并改善患者的护理和结局。