Department of Radiation Oncology, Tufts Medical Center, Box #593 800, Washington St, Boston, MA 02111, USA.
Radiat Oncol. 2012 May 18;7:72. doi: 10.1186/1748-717X-7-72.
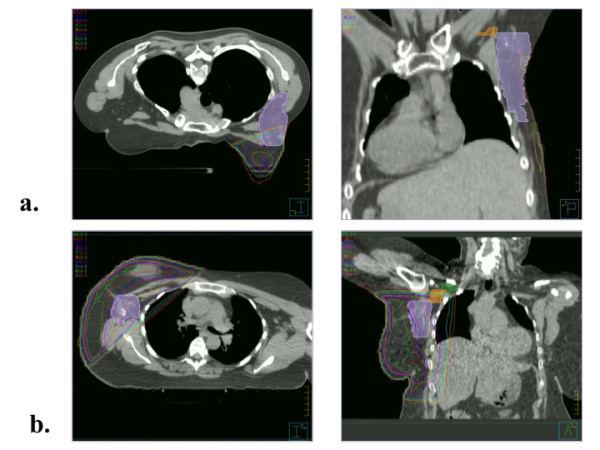
Prone breast positioning reduces skin reaction and heart and lung dose, but may also reduce radiation dose to axillary lymph nodes (ALNs).
Women with early stage breast cancer treated with whole breast irradiation (WBI) in the prone position were identified. Patients treated in the supine position were matched for treating physician, laterality, and fractionation. Ipsilateral breast, tumor bed, and Level I, II, and III ALNs were contoured according to the RTOG breast atlas. Clips marking surgically removed sentinel lymph nodes (SLN)s were contoured. Treatment plans developed for each patient were retrospectively analyzed. V90% and V95% was calculated for each axillary level. When present, dose to axillary surgical clips was calculated.
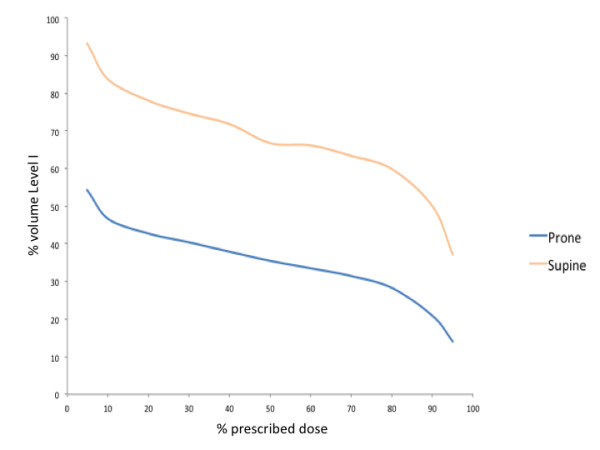
Treatment plans for 46 women (23 prone and 23 supine) were reviewed. The mean V90% and V95% of ALN Level I was significantly lower for patients treated in the prone position (21% and 14%, respectively) than in the supine position (50% and 37%, respectively) (p < 0.0001 and p < 0.0001, respectively). Generally, Level II & III ALNs received little dose in either position. Sentinel node biopsy clips were all contained within axillary Level I. The mean V95% of SLN clips was 47% for patients treated in the supine position and 0% for patients treated in the prone position (p < 0.0001). Mean V90% to SLN clips was 96% for women treated in the supine position but only 13% for women treated in the prone position.
Standard tangential breast irradiation in the prone position results in substantially reduced dose to the Level I axilla as compared with treatment in the supine position. For women in whom axillary coverage is indicated such as those with positive sentinel lymph node biopsy who do not undergo completion axillary dissection, treatment in the prone position may be inappropriate.
俯卧位乳房定位可减少皮肤反应和心肺剂量,但也可能降低腋窝淋巴结(ALN)的放射剂量。
确定了接受俯卧位全乳照射(WBI)治疗的早期乳腺癌患者。仰卧位治疗的患者按治疗医生、侧别和分割进行匹配。根据 RTOG 乳房图谱对同侧乳房、肿瘤床和 ALN 水平 I、II 和 III 进行轮廓勾画。对手术切除的前哨淋巴结(SLN)标记夹进行轮廓勾画。回顾性分析每位患者的治疗计划。计算每个腋窝水平的 V90%和 V95%。当存在时,计算腋窝手术夹的剂量。
共回顾了 46 名女性(23 名俯卧位和 23 名仰卧位)的治疗计划。与仰卧位相比,俯卧位治疗的 ALN 水平 I 的平均 V90%和 V95%明显更低(分别为 21%和 14%,分别为 50%和 37%)(p<0.0001 和 p<0.0001)。通常,两种体位下 II & III 水平的 ALN 接收的剂量都很少。前哨淋巴结活检夹均位于腋窝 I 水平内。仰卧位治疗患者的 SLN 夹平均 V95%为 47%,俯卧位治疗患者的 SLN 夹平均 V95%为 0%(p<0.0001)。仰卧位治疗的女性 SLN 夹的平均 V90%为 96%,而俯卧位治疗的女性 SLN 夹的平均 V90%仅为 13%。
与仰卧位治疗相比,标准切线乳房照射在俯卧位可显著降低 I 水平腋窝的剂量。对于需要腋窝覆盖的女性,如前哨淋巴结活检阳性但不进行完成腋窝清扫的女性,俯卧位治疗可能不合适。