Department of Medicine, Division of Hematology/Oncology, University of Miami/Sylvester Comprehensive Cancer Center, Miami, FL, USA.
BMC Cancer. 2012 May 29;12:199. doi: 10.1186/1471-2407-12-199.
5-fluorouracil, leucovorin, irinotecan and oxaliplatin (FOLFIRINOX) is superior to gemcitabine in patients with metastatic pancreatic cancer who have a good performance status. We investigated this combination as neoadjuvant therapy for locally advanced pancreatic cancer (LAPC).
In this retrospective series, we included patients with unresectable LAPC who received neoadjuvant FOLFIRINOX with growth factor support. The primary analysis endpoint was R0 resection rate.
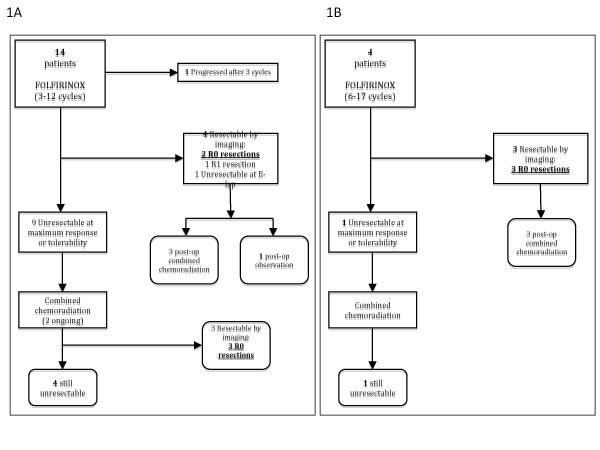
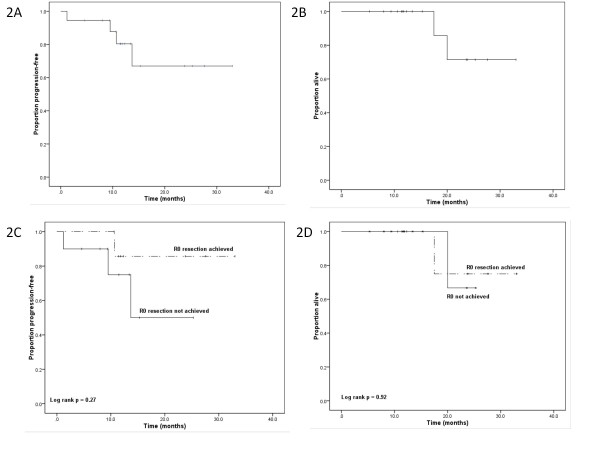
Eighteen treatment-naïve patients with unresectable or borderline resectable LAPC were treated with neoadjuvant FOLFIRINOX. The median age was 57.5 years and all had ECOG PS of 0 or 1. Eleven (61 %) had tumors in the head of the pancreas and 9 (50 %) had biliary stents placed prior to chemotherapy. A total of 146 cycles were administered with a median of 8 cycles (range 3-17) per patient. At maximum response or tolerability, 7 (39 %) were converted to resectability by radiological criteria; 5 had R0 resections, 1 had an R1 resection, and 1 had unresectable disease. Among the 11 patients who remained unresectable after FOLFIRINOX, 3 went on to have R0 resections after combined chemoradiotherapy, giving an overall R0 resection rate of 44 % (95 % CI 22-69 %). After a median follow-up of 13.4 months, the 1-year progression-free survival was 83 % (95 % CI 59-96 %) and the 1-year overall survival was 100 % (95 % CI 85-100 %). Grade 3/4 chemotherapy-related toxicities were neutropenia (22 %), neutropenic fever (17 %), thrombocytopenia (11 %), fatigue (11 %), and diarrhea (11 %). Common grade 1/2 toxicities were neutropenia (33 %), anemia (72 %), thrombocytopenia (44 %), fatigue (78 %), nausea (50 %), diarrhea (33 %) and neuropathy (33 %).
FOLFIRINOX followed by chemoradiotherapy is feasible as neoadjuvant therapy in patients with unresectable LAPC. The R0 resection rate of 44 % in this population is promising. Further studies are warranted.
5-氟尿嘧啶、亚叶酸钙、伊立替康和奥沙利铂(FOLFIRINOX)在体能状态良好的转移性胰腺癌患者中优于吉西他滨。我们研究了该联合方案作为局部晚期胰腺癌(LAPC)的新辅助治疗。
在这项回顾性研究中,我们纳入了接受新辅助 FOLFIRINOX 联合生长因子支持治疗的不可切除的局部晚期胰腺癌患者。主要分析终点是 R0 切除率。
18 例未经治疗的不可切除或边界可切除的局部晚期胰腺癌患者接受了新辅助 FOLFIRINOX 治疗。中位年龄为 57.5 岁,所有患者 ECOG PS 评分为 0 或 1。11 例(61%)肿瘤位于胰头部,9 例(50%)化疗前放置了胆道支架。中位每个患者接受了 8 个周期的治疗(范围为 3-17 个周期),共接受了 146 个周期。在最大反应或可耐受性时,根据影像学标准,有 7 例(39%)转化为可切除性;5 例患者获得 R0 切除,1 例患者获得 R1 切除,1 例患者疾病仍不可切除。在 FOLFIRINOX 后仍不可切除的 11 例患者中,3 例在联合放化疗后获得 R0 切除,总体 R0 切除率为 44%(95%CI 22-69%)。中位随访 13.4 个月后,1 年无进展生存率为 83%(95%CI 59-96%),1 年总生存率为 100%(95%CI 85-100%)。3/4 级化疗相关毒性为中性粒细胞减少症(22%)、中性粒细胞减少症发热(17%)、血小板减少症(11%)、疲劳(11%)和腹泻(11%)。常见的 1/2 级毒性为中性粒细胞减少症(33%)、贫血(72%)、血小板减少症(44%)、疲劳(78%)、恶心(50%)、腹泻(33%)和神经病变(33%)。
FOLFIRINOX 序贯放化疗可作为不可切除局部晚期胰腺癌的新辅助治疗方法。该人群中 44%的 R0 切除率令人鼓舞。需要进一步研究。