Ferrone Cristina R, Marchegiani Giovanni, Hong Theodore S, Ryan David P, Deshpande Vikram, McDonnell Erin I, Sabbatino Francesco, Santos Daniela Dias, Allen Jill N, Blaszkowsky Lawrence S, Clark Jeffrey W, Faris Jason E, Goyal Lipika, Kwak Eunice L, Murphy Janet E, Ting David T, Wo Jennifer Y, Zhu Andrew X, Warshaw Andrew L, Lillemoe Keith D, Fernández-del Castillo Carlos
*Department of Surgery †Department of Radiation Oncology; and ‡Department of Medical Oncology, Massachusetts General Hospital, Harvard Medical School, Boston, MA.
Ann Surg. 2015 Jan;261(1):12-7. doi: 10.1097/SLA.0000000000000867.
On the basis of the ACCORD trial, FOLFIRINOX is effective in metastatic pancreatic adenocarcinoma (PDAC), making it a rational choice for locally advanced PDAC (LA). Aims of this study are to evaluate the accuracy of imaging in determining the resectability of PDAC and to determine the surgical and clinicopathologic outcomes of pancreatic resections after neoadjuvant FOLFIRINOX therapy.
Clinicopathologic data were retrospectively collected for surgical PDAC patients receiving neoadjuvant FOLFIRINOX or no neoadjuvant therapy between April 2011 and February 2014. Americas Hepato-Pancreato-Biliary Association/Society of Surgical Oncology/Society for Surgery of the Alimentary Tract consensus guidelines defined LA and borderline. Imaging was reviewed by a blinded senior pancreatic surgeon.
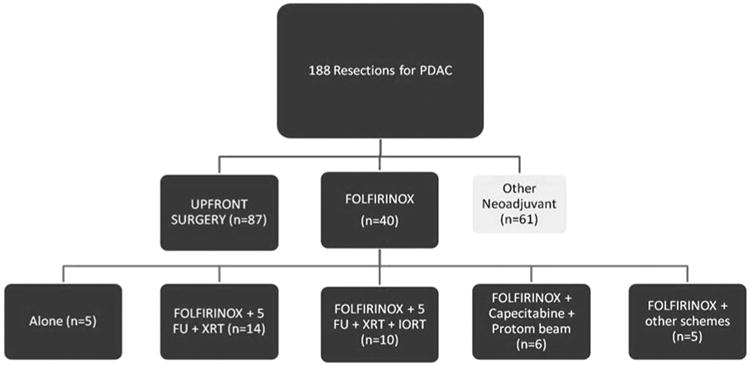
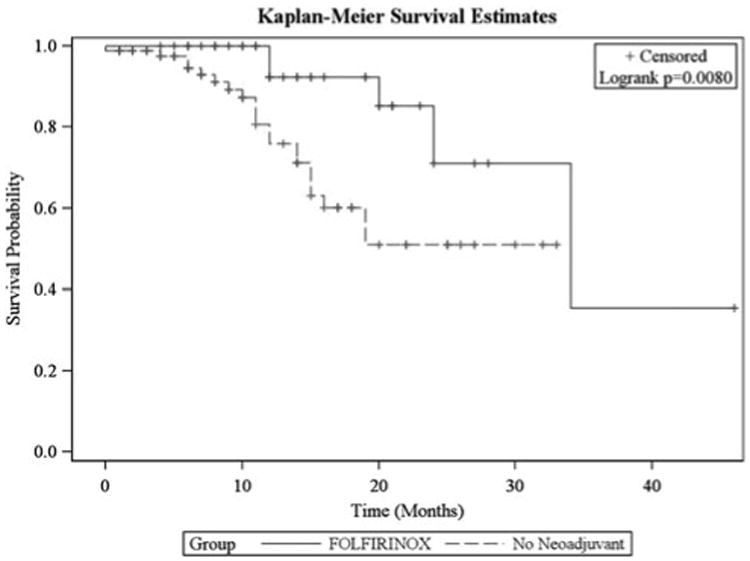
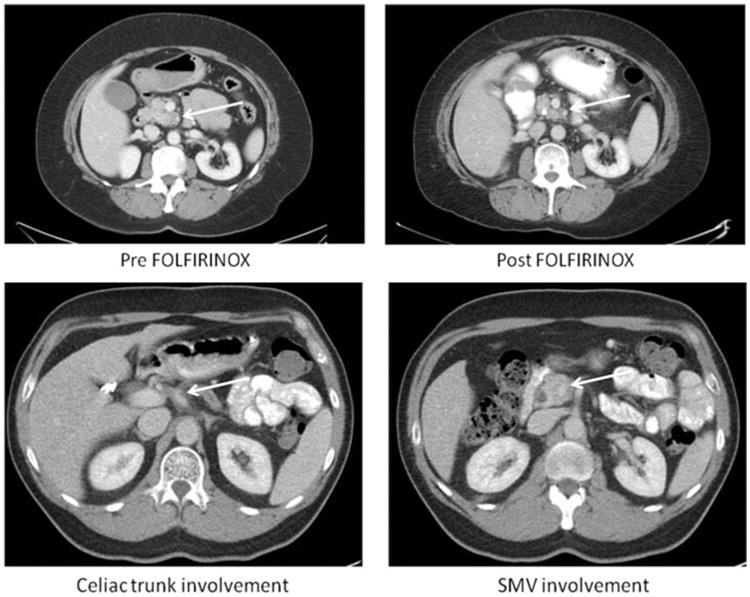
Of 188 patients undergoing resection for PDAC, 40 LA/borderline received FOLFIRINOX and 87 received no neoadjuvant therapy. FOLFIRINOX resulted in a significant decrease in tumor size, yet 19 patients were still classified as LA and 9 as borderline. Despite post-FOLFIRINOX imaging suggesting continued unresectability, 92% had an R0 resection. When compared with no neoadjuvant therapy, FOLFIRINOX resulted in significantly longer operative times (393 vs 300 minutes) and blood loss (600 vs 400 mL), but significantly lower operative morbidity (36% vs 63%) and no postoperative pancreatic fistulas. Length of stay (6 vs 7 days), readmissions (20% vs 30%), and mortality were equivalent (1% vs 0%). On final pathology, the FOLFIRINOX group had a significant decrease in lymph node positivity (35% vs 79%) and perineural invasion (72% vs 95%). Median follow-up was 11 months with a significant increase in overall survival with FOLFIRINOX.
After neoadjuvant FOLFIRINOX imaging no longer predicts unresectability. Traditional pathologic predictors of survival are improved, and morbidity is decreased in comparison to patients with clearly resectable cancers at the time of presentation.
基于ACCORD试验,FOLFIRINOX方案对转移性胰腺腺癌(PDAC)有效,使其成为局部晚期PDAC(LA)的合理选择。本研究的目的是评估影像学在确定PDAC可切除性方面的准确性,并确定新辅助FOLFIRINOX治疗后胰腺切除术的手术及临床病理结果。
回顾性收集2011年4月至2014年2月间接受新辅助FOLFIRINOX治疗或未接受新辅助治疗的手术治疗PDAC患者的临床病理数据。美洲肝脏胰胆协会/外科肿瘤学会/消化道外科学会共识指南定义了LA和临界状态。由一位不知情的资深胰腺外科医生复查影像学资料。
188例接受PDAC切除术的患者中,40例LA/临界状态患者接受了FOLFIRINOX治疗,87例未接受新辅助治疗。FOLFIRINOX治疗使肿瘤大小显著减小,但仍有19例患者被归类为LA,9例为临界状态。尽管FOLFIRINOX治疗后的影像学检查提示仍不可切除,但92%的患者实现了R0切除。与未接受新辅助治疗相比,FOLFIRINOX治疗导致手术时间显著延长(393分钟对300分钟)和失血量增加(600毫升对400毫升),但手术并发症显著降低(36%对63%)且无术后胰瘘。住院时间(6天对7天)、再入院率(20%对30%)和死亡率相当(1%对0%)。在最终病理检查中,FOLFIRINOX组淋巴结阳性率(35%对79%)和神经周围侵犯率(72%对95%)显著降低。中位随访时间为11个月,FOLFIRINOX治疗使总生存期显著延长。
新辅助FOLFIRINOX治疗后,影像学不再能预测不可切除性。与初诊时明确可切除的癌症患者相比,传统的生存病理预测指标得到改善,并发症减少。