Department of Internal Medicine I, Martin-Luther-University Halle-Wittenberg, Halle, Germany.
Liver Int. 2012 Oct;32(9):1407-14. doi: 10.1111/j.1478-3231.2012.02830.x. Epub 2012 Jun 11.
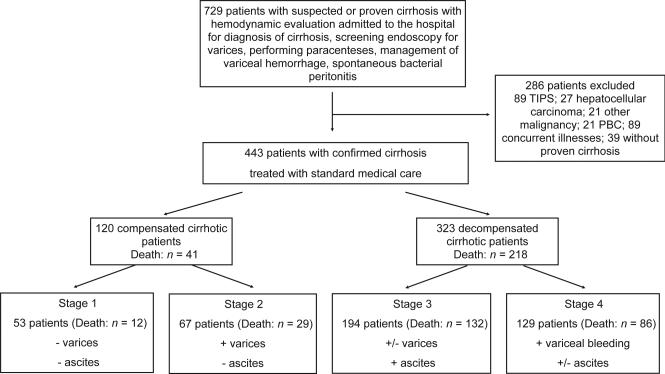
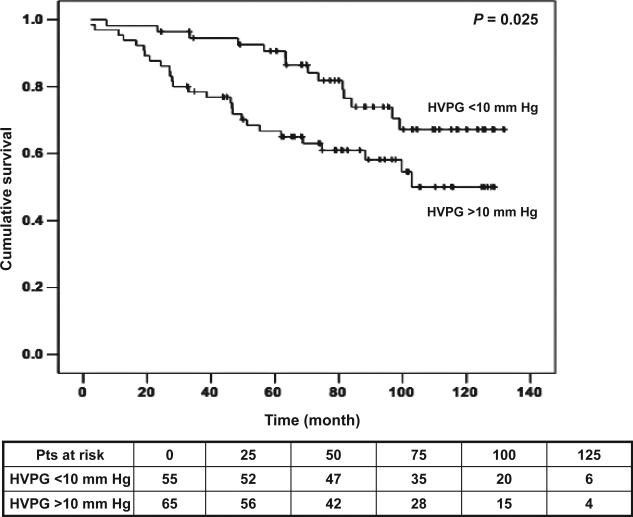
BACKGROUND/AIMS: Patients with cirrhosis are classified in a compensated and a decompensated stage. Portal hypertension is responsible for most of the complications of cirrhosis that mark the transition from compensated to decompensated cirrhosis. The objectives of this study were (a) to analyse survival of the different stages and substages of cirrhosis and (b) to examine the prognostic value of the hepatic venous pressure gradient (HVPG) at each of the stages.
A total of 729 patients with suspected cirrhosis underwent routine measurement of portal pressure and systemic haemodynamics between 11/1995 and 12/2004. The primary end-point of the study was death, collected until November 30th, 2006. Multivariable analysis was performed using two models to determine predictors of death at each stage.
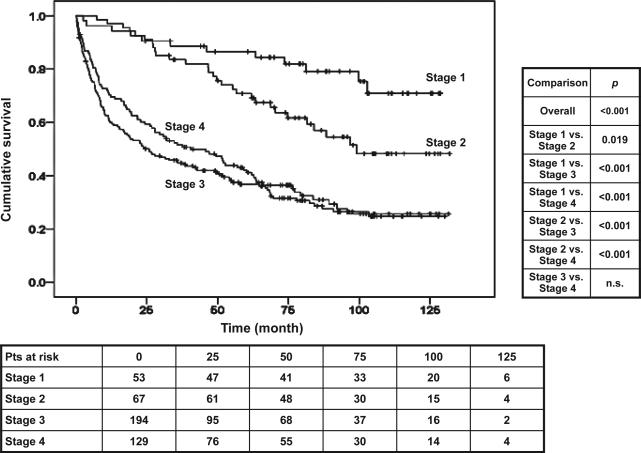
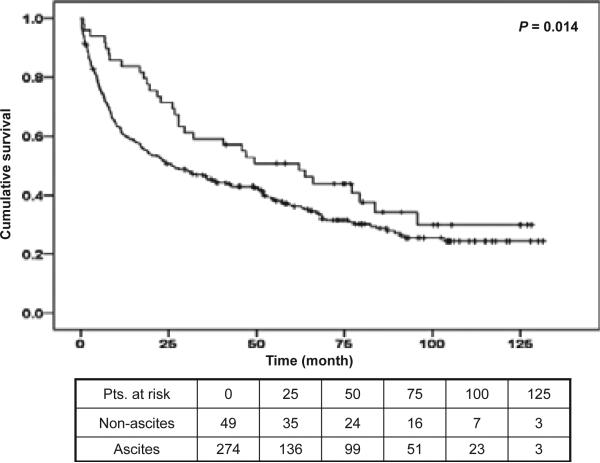
A total of 443 patients were included in the study. The 1-year mortality was 5.4% in compensated and 20.2% in decompensated patients. Compensated patients in stage 1 (no varices) had a longer survival than stage 2 patients (varices present) (P = 0.015). In decompensated patients, survival was not different between stage 3 (ascites, with or without varices) and stage 4 (variceal haemorrhage, with or without ascites). Age and HVPG (cut-off 10 mmHg) were independent predictors of death in compensated patients, whereas MELD was in decompensated patients.
Survival rates and predictors of death are different between patients with compensated and decompensated cirrhosis. Unlike the Italian cohort staging system, ascites is a better stratifying clinical event than variceal haemorrhage in patients with decompensated cirrhosis. The presence of clinically significant portal hypertension has prognostic value in compensated cirrhosis.
背景/目的:肝硬化患者分为代偿期和失代偿期。门静脉高压是肝硬化大多数并发症的原因,这些并发症标志着从代偿期向失代偿期肝硬化的转变。本研究的目的是:(a)分析不同阶段和亚阶段肝硬化的生存率;(b)检查肝静脉压力梯度(HVPG)在各阶段的预后价值。
1995 年 11 月至 2004 年 12 月,共有 729 例疑似肝硬化患者接受常规门静脉压力和全身血液动力学测量。本研究的主要终点是死亡,直到 2006 年 11 月 30 日收集。使用两种模型进行多变量分析,以确定各阶段死亡的预测因素。
共有 443 例患者纳入本研究。代偿期患者 1 年死亡率为 5.4%,失代偿期患者为 20.2%。代偿期 1 期(无静脉曲张)患者的生存率长于 2 期(有静脉曲张)患者(P=0.015)。在失代偿期患者中,3 期(腹水,有或无静脉曲张)和 4 期(静脉曲张出血,有或无腹水)患者的生存率无差异。年龄和 HVPG(截断值 10mmHg)是代偿期患者死亡的独立预测因素,而 MELD 是失代偿期患者的独立预测因素。
代偿期和失代偿期肝硬化患者的生存率和死亡预测因素不同。与意大利队列分期系统不同,腹水是失代偿期肝硬化患者比静脉曲张出血更好的分层临床事件。临床显著门静脉高压的存在对代偿期肝硬化具有预后价值。