Department of Dermatology, University Hospital of Regensburg, Regensburg, Germany.
PLoS One. 2012;7(6):e38222. doi: 10.1371/journal.pone.0038222. Epub 2012 Jun 7.
Current staging methods such as tumor thickness, ulceration and invasion of the sentinel node are known to be prognostic parameters in patients with malignant melanoma (MM). However, predictive molecular marker profiles for risk stratification and therapy optimization are not yet available for routine clinical assessment.
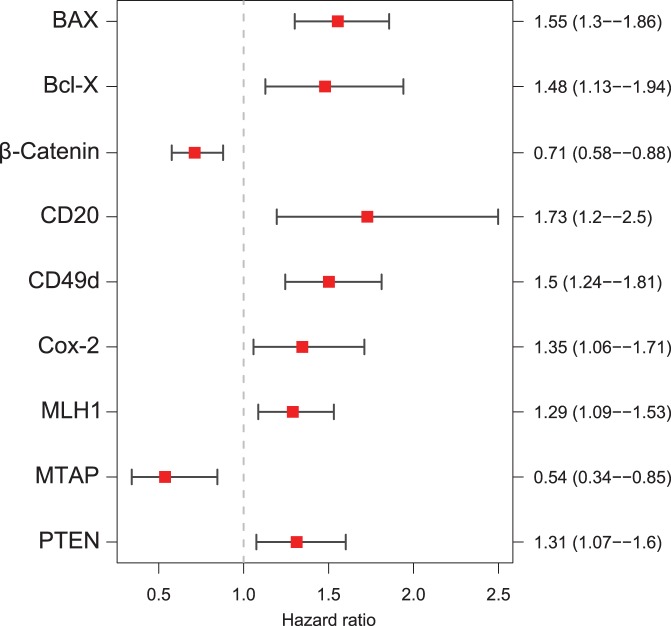
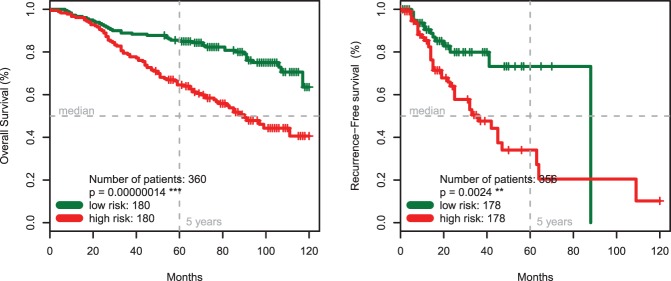
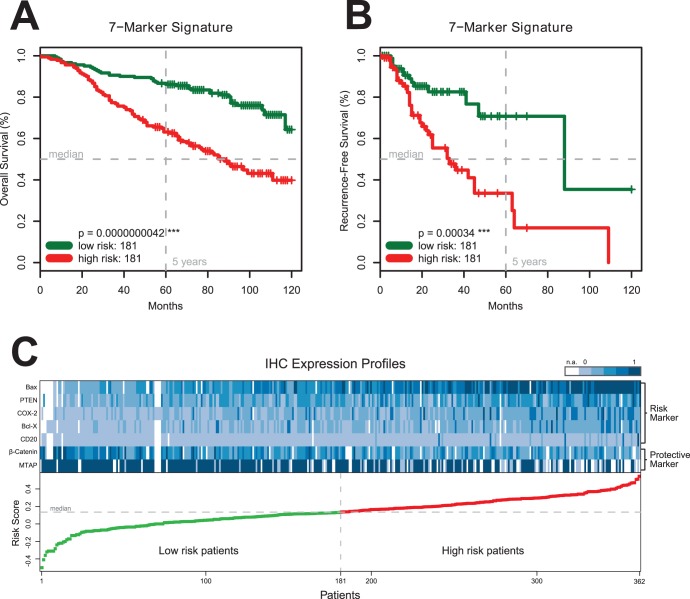
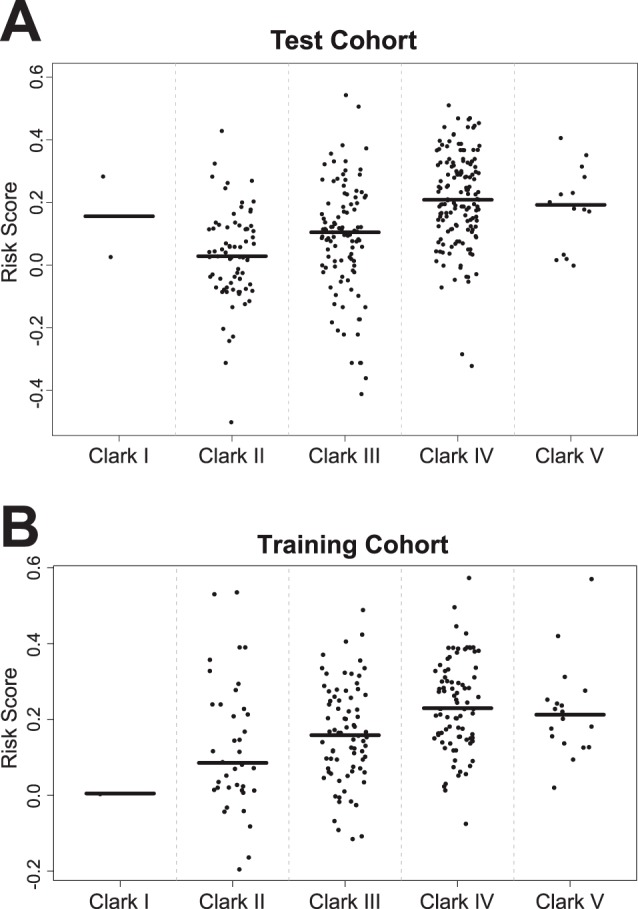
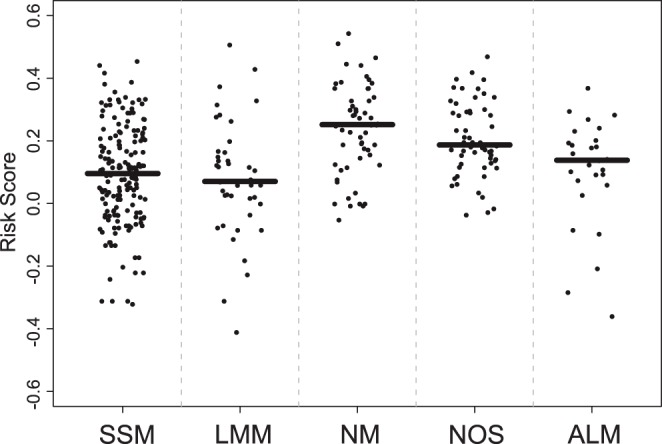
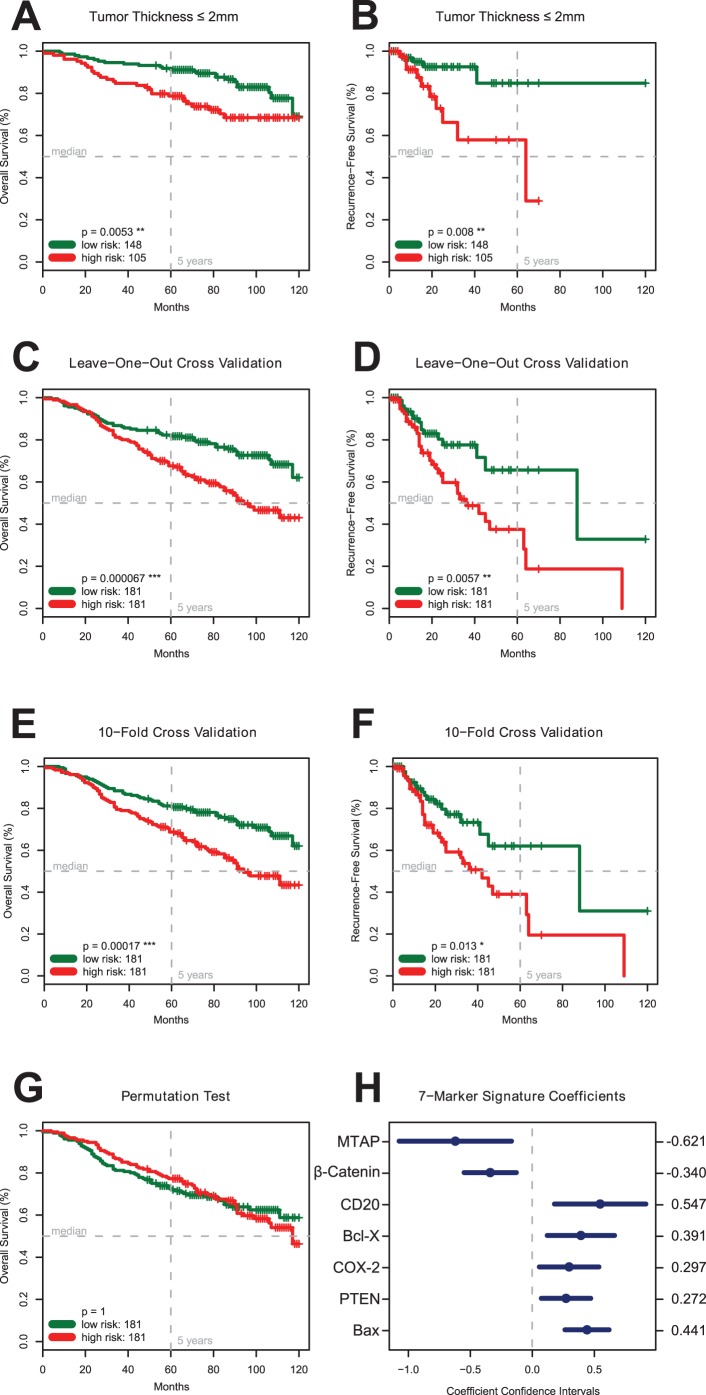
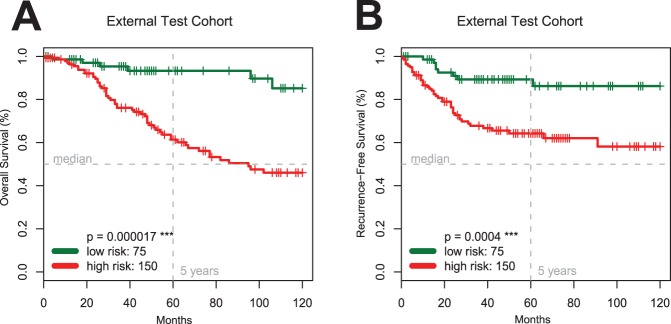
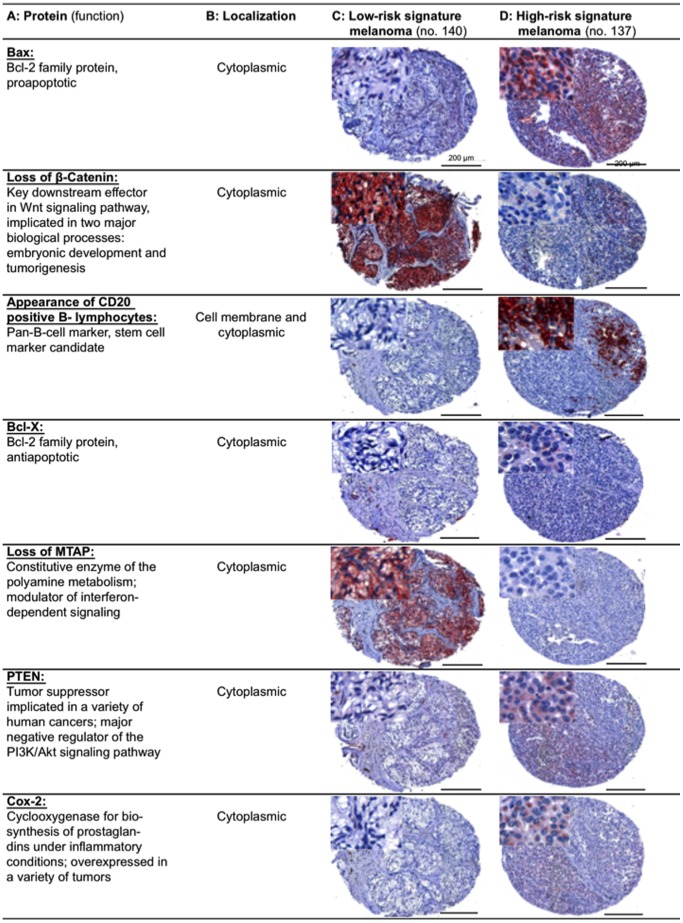
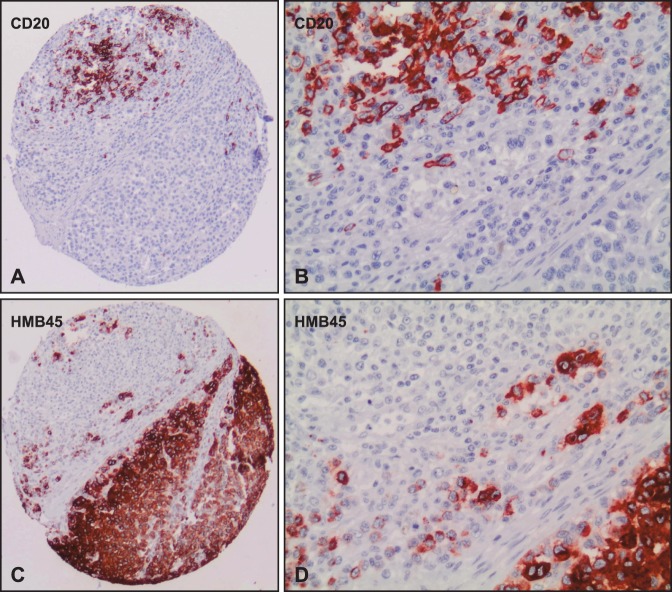
Using tissue microarrays, we retrospectively analyzed samples from 364 patients with primary MM. We investigated a panel of 70 immunohistochemical (IHC) antibodies for cell cycle, apoptosis, DNA mismatch repair, differentiation, proliferation, cell adhesion, signaling and metabolism. A marker selection procedure based on univariate Cox regression and multiple testing correction was employed to correlate the IHC expression data with the clinical follow-up (overall and recurrence-free survival). The model was thoroughly evaluated with two different cross validation experiments, a permutation test and a multivariate Cox regression analysis. In addition, the predictive power of the identified marker signature was validated on a second independent external test cohort (n=225). A signature of seven biomarkers (Bax, Bcl-X, PTEN, COX-2, loss of β-Catenin, loss of MTAP, and presence of CD20 positive B-lymphocytes) was found to be an independent negative predictor for overall and recurrence-free survival in patients with MM. The seven-marker signature could also predict a high risk of disease recurrence in patients with localized primary MM stage pT1-2 (tumor thickness ≤2.00 mm). In particular, three of these markers (MTAP, COX-2, Bcl-X) were shown to offer direct therapeutic implications.
The seven-marker signature might serve as a prognostic tool enabling physicians to selectively triage, at the time of diagnosis, the subset of high recurrence risk stage I-II patients for adjuvant therapy. Selective treatment of those patients that are more likely to develop distant metastatic disease could potentially lower the burden of untreatable metastatic melanoma and revolutionize the therapeutic management of MM.
目前,肿瘤厚度、溃疡和前哨淋巴结浸润等分期方法已被证实是恶性黑色素瘤(MM)患者的预后参数。然而,用于风险分层和治疗优化的预测性分子标志物谱尚不能用于常规临床评估。
我们使用组织微阵列,回顾性分析了 364 例原发性 MM 患者的样本。我们研究了 70 种免疫组织化学(IHC)抗体的面板,用于细胞周期、凋亡、DNA 错配修复、分化、增殖、细胞黏附、信号转导和代谢。采用基于单变量 Cox 回归和多重检验校正的标记选择程序,将 IHC 表达数据与临床随访(总生存和无复发生存)相关联。该模型通过两个不同的交叉验证实验、置换检验和多变量 Cox 回归分析进行了全面评估。此外,还在第二个独立的外部测试队列(n=225)上验证了鉴定的标志物特征的预测能力。发现七种生物标志物(Bax、Bcl-X、PTEN、COX-2、β-Catenin 缺失、MTAP 缺失和 CD20 阳性 B 淋巴细胞存在)的特征是 MM 患者总生存和无复发生存的独立负预测因子。该七种标志物特征还可以预测局部原发性 MM 期 pT1-2(肿瘤厚度≤2.00mm)患者疾病复发的高风险。特别是,其中三种标志物(MTAP、COX-2、Bcl-X)被证明具有直接的治疗意义。
七种标志物特征可能作为一种预后工具,使医生能够在诊断时选择性地对高复发风险的 I-II 期患者进行辅助治疗。对那些更有可能发生远处转移性疾病的患者进行选择性治疗,可能会降低无法治疗的转移性黑色素瘤的负担,并彻底改变 MM 的治疗管理。