Bell April J, Wools-Kaloustian Kara, Kimaiyo Sylvester, Liu Hai, Katschke Adrian, Shen Changyu, Simiyu Gilbert, Musick Beverly S, Sidle John E, Siika Abraham, Braitstein Paula
Indiana University School of Medicine, 1001 West 10th Street, OPW M200, Indianapolis, IN 46202, USA.
AIDS Res Treat. 2012;2012:814564. doi: 10.1155/2012/814564. Epub 2012 May 29.
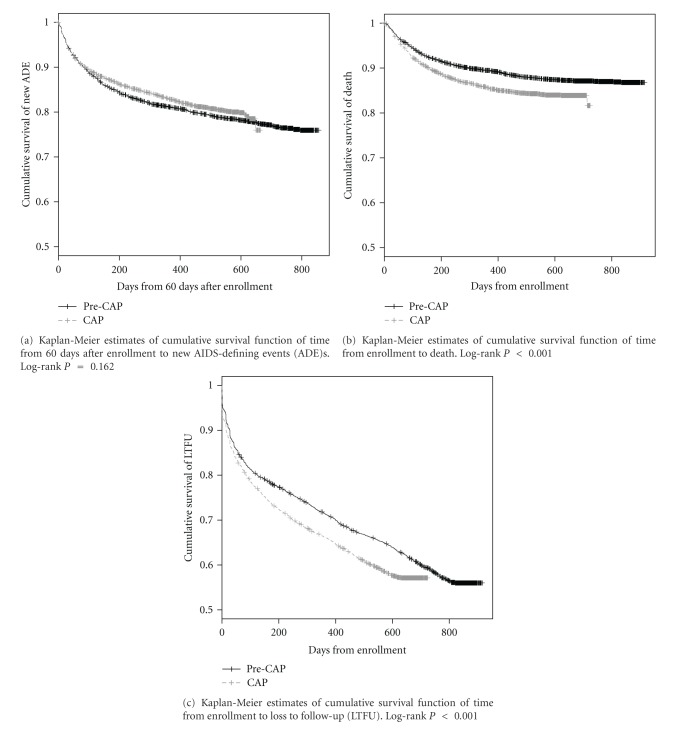
Background. There was a 6-month shortage of antiretrovirals (cART) in Kenya. Methods. We assessed morbidity, mortality, and loss to follow-up (LTFU) in this retrospective analysis of adults who were enrolled during the six-month period with restricted cART (cap) or the six months prior (pre-cap) and eligible for cART at enrollment by the pre-cap standard. Cox models were used to adjust for potential confounders. Results. 9009 adults were eligible for analysis: 4,714 pre-cap and 4,295 during the cap. Median number of days from enrollment to cART initiation was 42 pre-cap and 56 for the cap (P < 0.001). After adjustment, individuals in the cap were at higher risk of mortality (HR = 1.21; 95% CI : 1.06-1.39) and LTFU (HR = 1.12; 95% CI : 1.04-1.22). There was no difference between the groups in their risk of developing a new AIDS-defining illness (HR = 0.92 95% CI 0.82-1.03). Conclusions. Rationing of cART, even for a relatively short period of six months, led to clinically adverse outcomes.
背景。肯尼亚曾出现抗逆转录病毒药物(cART)短缺6个月的情况。方法。在这项回顾性分析中,我们评估了在cART供应受限的6个月期间(cap)或此前6个月(cap前)入组且根据cap前标准入组时符合cART治疗条件的成年人的发病率、死亡率和失访情况。使用Cox模型对潜在混杂因素进行调整。结果。9009名成年人符合分析条件:cap前组4714人,cap组4295人。从入组到开始cART治疗的中位天数,cap前组为42天,cap组为56天(P < 0.001)。调整后,cap组个体的死亡风险(HR = 1.21;95% CI:1.06 - 1.39)和失访风险(HR = 1.12;95% CI:1.04 - 1.22)更高。两组在发生新的艾滋病定义疾病的风险方面没有差异(HR = 0.92,95% CI 0.82 - 1.03)。结论。即使cART供应受限仅6个月这样相对较短的时间,也会导致临床不良后果。