Department of Obstetrics and Gynaecology, Leuven Cancer Institute, Universitaire Ziekenhuizen Leuven, KU Leuven, Herestraat 49, 3000, Leuven, Belgium.
Proteome Sci. 2012 Jun 13;10(1):41. doi: 10.1186/1477-5956-10-41.
Lymph node status is not part of the staging system for cervical cancer, but provides important information for prognosis and treatment. We investigated whether lymph node status can be predicted with proteomic profiling.
MATERIAL & METHODS: Serum samples of 60 cervical cancer patients (FIGO I/II) were obtained before primary treatment. Samples were run through a HPLC depletion column, eliminating the 14 most abundant proteins ubiquitously present in serum. Unbound fractions were concentrated with spin filters. Fractions were spotted onto CM10 and IMAC30 surfaces and analyzed with surface-enhanced laser desorption time of flight (SELDI-TOF) mass spectrometry (MS). Unsupervised peak detection and peak clustering was performed using MASDA software. Leave-one-out (LOO) validation for weighted Least Squares Support Vector Machines (LSSVM) was used for prediction of lymph node involvement. Other outcomes were histological type, lymphvascular space involvement (LVSI) and recurrent disease.
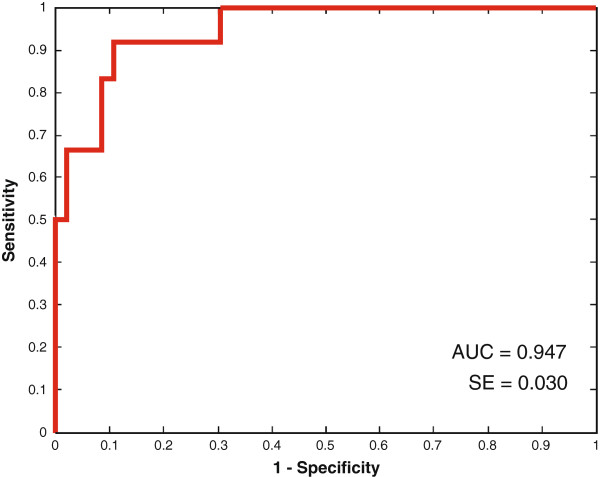
LSSVM models were able to determine LN status with a LOO area under the receiver operating characteristics curve (AUC) of 0.95, based on peaks with m/z values 2,698.9, 3,953.2, and 15,254.8. Furthermore, we were able to predict LVSI (AUC 0.81), to predict recurrence (AUC 0.92), and to differentiate between squamous carcinomas and adenocarcinomas (AUC 0.88), between squamous and adenosquamous carcinomas (AUC 0.85), and between adenocarcinomas and adenosquamous carcinomas (AUC 0.94).
Potential markers related with lymph node involvement were detected, and protein/peptide profiling support differentiation between various subtypes of cervical cancer. However, identification of the potential biomarkers was hampered by the technical limitations of SELDI-TOF MS.
淋巴结状态不是宫颈癌分期系统的一部分,但为预后和治疗提供了重要信息。我们研究了蛋白质组谱是否可以预测淋巴结状态。
60 例宫颈癌患者(FIGO I/II 期)在初次治疗前采集血清样本。样本通过 HPLC 耗尽柱进行处理,去除普遍存在于血清中的 14 种最丰富的蛋白质。未结合的部分用自旋过滤器浓缩。将各部分点样到 CM10 和 IMAC30 表面,用表面增强激光解吸飞行时间(SELDI-TOF)质谱(MS)进行分析。使用 MASDA 软件进行非监督峰检测和峰聚类。使用加权最小二乘支持向量机(LSSVM)进行的留一法(LOO)验证用于预测淋巴结受累。其他结果包括组织学类型、淋巴血管空间侵犯(LVSI)和复发性疾病。
LSSVM 模型能够基于质荷比(m/z)值为 2,698.9、3,953.2 和 15,254.8 的峰,以 LOO 受试者工作特征曲线(ROC)下面积 0.95 确定 LN 状态。此外,我们能够预测 LVSI(AUC 0.81)、预测复发(AUC 0.92),以及区分鳞癌和腺癌(AUC 0.88)、鳞癌和腺鳞癌(AUC 0.85),以及腺癌和腺鳞癌(AUC 0.94)。
检测到与淋巴结受累相关的潜在标志物,并且蛋白质/肽谱支持对不同类型的宫颈癌进行区分。然而,SELDI-TOF MS 的技术限制阻碍了潜在生物标志物的识别。