Arvaniti Kostoula, Lathyris Dimitrios, Ruimy Raymond, Haidich Anna-Bettina, Koulourida Vasiliki, Nikolaidis Pavlos, Matamis Dimitrios, Miyakis Spiros
Crit Care. 2012 Jun 13;16(3):R102. doi: 10.1186/cc11383.
We investigated the role of colonization pressure on multiresistant Acinetobacter baumannii acquisition and defined patient-related predictors for carriage at admission and acquisition during hospitalization in intensive care unit (ICU) patients.
This was a 12-month, prospective, cohort study of all patients admitted to a single ICU of a tertiary hospital. Screening samples were collected at ICU admission to identify imported carriers, and weekly during hospitalization to identify acquisition. Colonization pressure (carriers' patient-days × 100/all patients' patient-days) and the absolute number of carriers were calculated weekly, and the statistical correlation between these parameters and acquisition was explored. Multivariable analysis was performed to identify predictors for A. baumannii carriage at admission and acquisition during hospitalization. A. baumannii isolates were genotyped by repetitive-extragenic-palindromic polymerase chain reaction (PCR; rep-PCR).
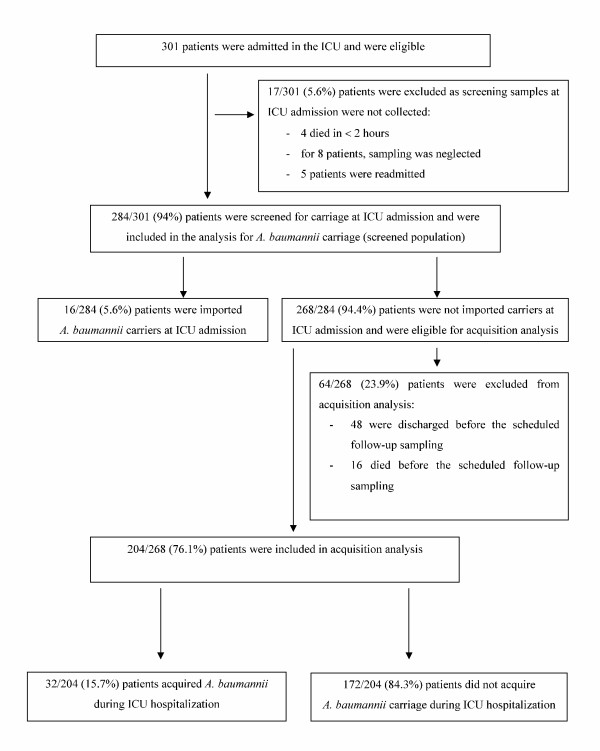
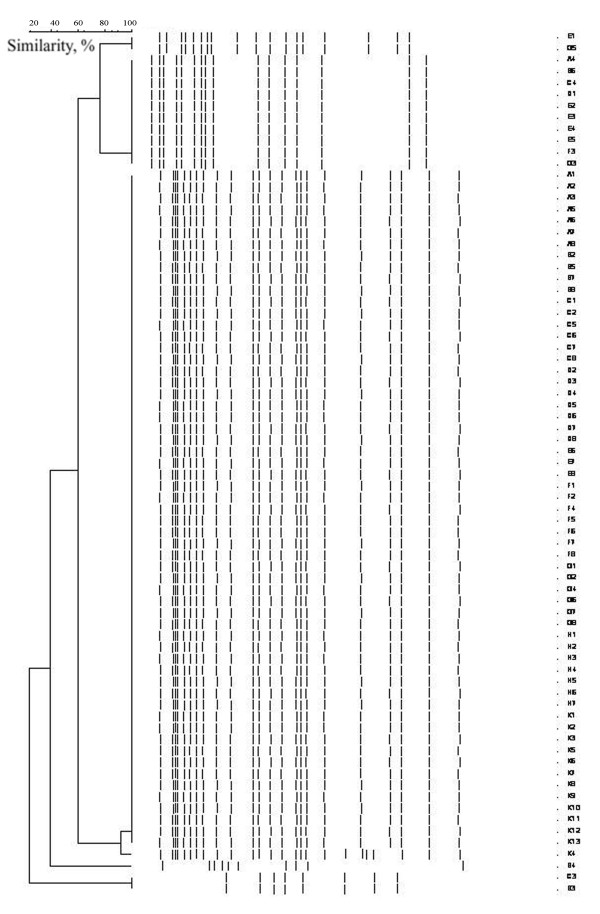
At ICU admission, 284 patients were screened for carriage. A. baumannii was imported in 16 patients (5.6%), and acquisition occurred in 32 patients (15.7%). Acquisition was significantly correlated to weekly colonization pressure (correlation coefficient, 0.379; P = 0.004) and to the number of carriers per week (correlation coefficient, 0.499; P <0.001). More than one carrier per week significantly increased acquisition risk (two to three carriers, odds ratio (OR), 12.66; P = 0.028; more than four carriers, OR, 25.33; P = 0.004). Predictors of carriage at admission were infection at admission (OR, 11.03; confidence interval (CI), 3.56 to 34.18; P < 0.01) and hospitalization days before ICU (OR, 1.09; CI, 1.01 to 1.16; P = 0.02). Predictors of acquisition were a medical reason for ICU admission (OR, 5.11; CI, 1.31 to 19.93; P = 0.02), duration of antibiotic administration in the unit (OR, 1.24; CI, 1.12 to 1.38; P < 0.001), and duration of mechanical ventilation (OR, 1.08; CI, 1.04 to 1.13; P = 0.001). All strains were multiresistant. Rep-PCR analysis showed one dominant cluster.
Acquisition of multiresistant A. baumannii in ICU patients is strongly correlated to colonization pressure. High levels of colonization pressure and more than two carriers per week independently increase acquisition risk. Patient-related factors, such as infection at admission and long hospitalization before the ICU, can identify imported A. baumannii carriers. Medical patients with extended administration of antibiotics and long duration of mechanical ventilation in the ICU were the most vulnerable to acquisition.
我们研究了定植压力对多重耐药鲍曼不动杆菌感染的作用,并确定了重症监护病房(ICU)患者入院时携带该菌及住院期间感染的患者相关预测因素。
这是一项针对一家三级医院单个ICU所有入院患者的为期12个月的前瞻性队列研究。在ICU入院时采集筛查样本以识别输入性携带者,并在住院期间每周采集样本以识别感染情况。每周计算定植压力(携带者的患者日数×100/所有患者的患者日数)和携带者绝对数量,并探讨这些参数与感染之间的统计相关性。进行多变量分析以确定入院时鲍曼不动杆菌携带及住院期间感染的预测因素。通过重复外源性回文聚合酶链反应(PCR;rep-PCR)对鲍曼不动杆菌分离株进行基因分型。
在ICU入院时,对284例患者进行了携带情况筛查。16例患者(5.6%)输入了鲍曼不动杆菌,32例患者(15.7%)发生了感染。感染与每周定植压力显著相关(相关系数,0.379;P = 0.004)以及与每周携带者数量相关(相关系数,0.499;P <0.001)。每周有多于一名携带者显著增加感染风险(两名至三名携带者,比值比(OR),12.66;P = 0.028;多于四名携带者,OR,25.33;P = 0.004)。入院时携带的预测因素为入院时感染(OR,11.03;置信区间(CI),3.56至34.18;P < 0.01)以及ICU前住院天数(OR,1.09;CI,1.01至1.16;P = 0.02)。感染的预测因素为因医疗原因入住ICU(OR,5.11;CI,1.31至19.93;P = 0.02)、在该科室使用抗生素的持续时间(OR,1.24;CI,1.12至1.38;P < 0.001)以及机械通气持续时间(OR,1.08;CI,1.04至1.13;P = 0.001)。所有菌株均为多重耐药。Rep-PCR分析显示一个优势簇。
ICU患者多重耐药鲍曼不动杆菌的感染与定植压力密切相关。高水平的定植压力以及每周多于两名携带者会独立增加感染风险。患者相关因素,如入院时感染和ICU前长时间住院,可识别输入性鲍曼不动杆菌携带者。在ICU中使用抗生素时间延长且机械通气持续时间长的内科患者最易感染。