Department of Urologic Surgery, Vanderbilt University School of Medicine, Nashville, Tennessee 37232, USA.
J Urol. 2012 Aug;188(2):391-7. doi: 10.1016/j.juro.2012.04.006. Epub 2012 Jun 13.
Previous studies of the impact of renal cell carcinoma histopathology on survival are conflicting and generally limited to institutional analyses. Thus, we determined the role of renal cell carcinoma histopathology on the stage specific survival rate in a large population based cohort.
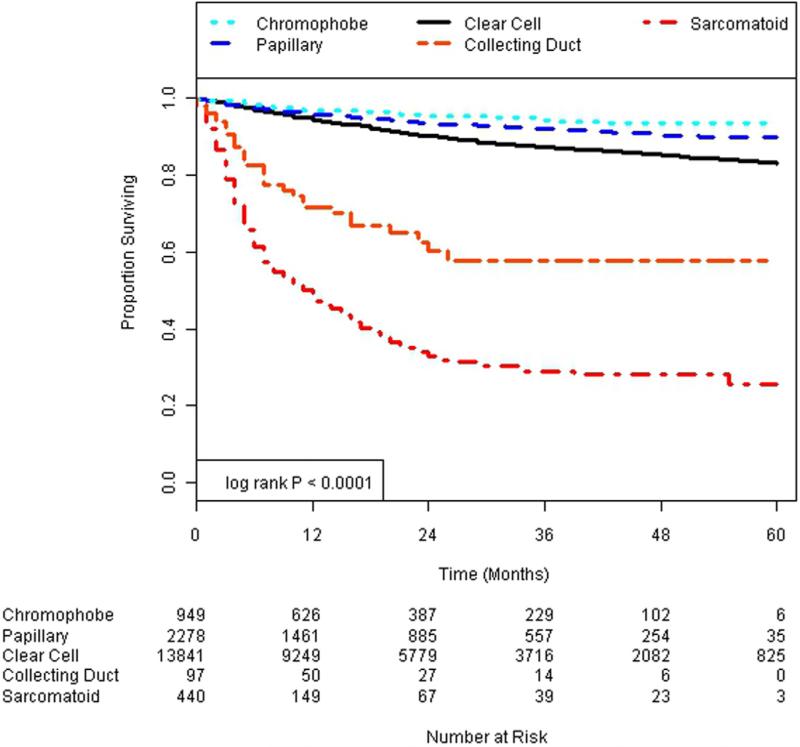
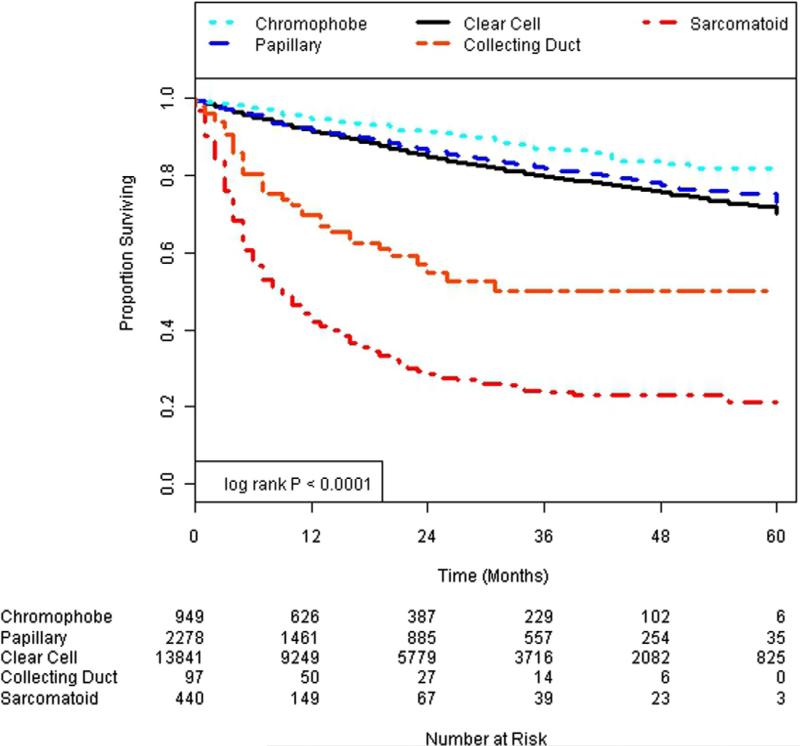
We used the 2000 to 2005 National Cancer Institute SEER (Surveillance, Epidemiology and End Results) database to identify 17,605 patients who underwent surgery for renal cell carcinoma and met study inclusion criteria. Patients were stratified by histological subtype (clear cell, papillary, chromophobe, collecting duct and sarcomatoid differentiation) and pathological stage. We performed Cox proportional hazard modeling and Kaplan-Meier survival analysis to determine overall and cancer specific survival.
Patients with papillary and chromophobe pathology were less likely to present with T3 or greater disease (17.6% and 16.9%, respectively) while patients with collecting duct and sarcomatoid variants were more likely to present with T3 or greater disease (55.7% and 82.8%, respectively) compared to those with clear cell histology (p <0.001). On multivariate analysis histology was significantly associated with overall and cancer specific survival. Patients with chromophobe pathology had improved survival (HR 0.56, 95% CI 0.40-0.78) while those with collecting duct and sarcomatoid variants had worse survival (HR 2.07, 95% CI 1.44-2.97 and 2.26, 95% CI 1.93-2.64, respectively).
Renal cell carcinoma histological subtype predicts overall and cancer specific survival. Patients with collecting duct and sarcomatoid variants of renal cell carcinoma have poor survival, even those who present with low stage disease. These data suggest inherent differences in renal cell carcinoma biology and may ultimately form the basis of future histologically targeted therapies.
先前关于肾细胞癌组织病理学对生存影响的研究结果存在争议,且通常仅限于机构分析。因此,我们旨在通过大样本人群队列研究来确定肾细胞癌组织病理学在特定分期的生存率中的作用。
我们使用了 2000 年至 2005 年美国国家癌症研究所 SEER(监测、流行病学和最终结果)数据库,共识别出 17605 例接受肾细胞癌手术且符合研究纳入标准的患者。根据组织学亚型(透明细胞、乳头状、嫌色细胞、集合管和肉瘤样分化)和病理分期对患者进行分层。我们进行了 Cox 比例风险模型和 Kaplan-Meier 生存分析,以确定总生存率和癌症特异性生存率。
与透明细胞组织学相比,具有乳头状和嫌色细胞组织学的患者不太可能出现 T3 或更高分期的疾病(分别为 17.6%和 16.9%),而具有集合管和肉瘤样变体的患者更有可能出现 T3 或更高分期的疾病(分别为 55.7%和 82.8%)(p<0.001)。多变量分析表明,组织学与总生存率和癌症特异性生存率显著相关。具有嫌色细胞组织学的患者的生存状况得到改善(HR 0.56,95%CI 0.40-0.78),而具有集合管和肉瘤样变体的患者的生存状况较差(HR 2.07,95%CI 1.44-2.97 和 2.26,95%CI 1.93-2.64)。
肾细胞癌的组织学亚型可预测总生存率和癌症特异性生存率。具有集合管和肉瘤样变体的肾细胞癌患者的生存状况较差,即使是那些出现低分期疾病的患者也是如此。这些数据表明肾细胞癌生物学存在固有差异,最终可能成为未来组织学靶向治疗的基础。