Altintas Nejat, Aslan Ekrem, Helvaci Aysen, Malhotra Atul
School of Medicine, Department of Pulmonary and Sleep Medicine, Mayis University, Samsun, Turkey.
Ann Saudi Med. 2012 Jul-Aug;32(4):384-90. doi: 10.5144/0256-4947.2012.384.
Obstructive sleep apnea (OSA) causes increased cardiovascular morbidity and mortality, including systemic arterial hypertension, coronary heart disease, heart rhythm and conduction disorders, heart failure and stroke. In our study, we aimed to assess left ventricular mass and myocardial performance index (MPI) in OSA patients.
A cross-sectional study conducted between May 2007 and August 2009 in a tertiary hospital in Istanbul, Turkey.
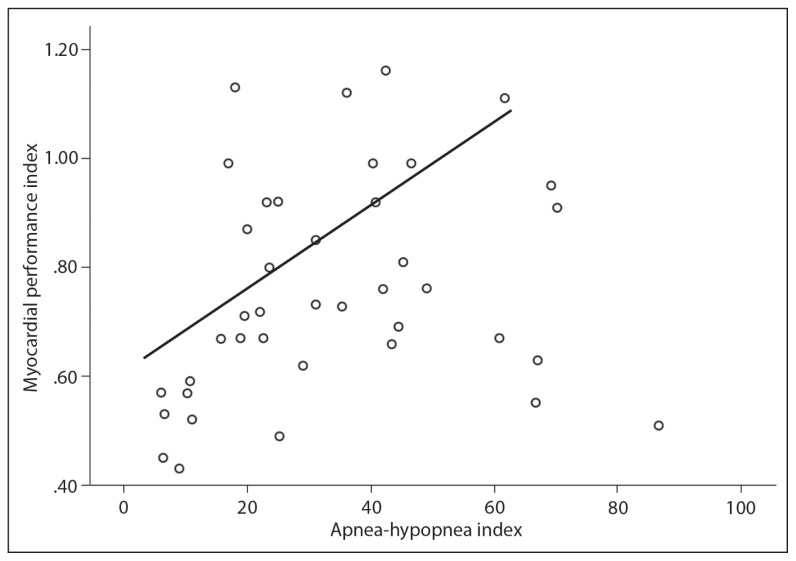
Forty subjects without any cardiac or pulmonary disease referred for evaluation of OSA had overnight polysomnography and echocardiography. According to the apnea-hypopnea index (AHI), subjects were classified into three groups; mild OSA (AHI: 5-14/h; n=7), moderate OSA (AHI: 15-29/h; n=13), and severe OSA (AHI: ;ge;30/h; n=20). The thickness of the interventricular septum (IVS) and left ventricular posterior wall (LVPW) were measured by M-mode along with left ventricular mass (LVM) and LVM index (LVMI). The left ventricular MPI was calculated as (isovolumic contraction time + isovolumic relaxation time)/aortic ejection time by Doppler echocardiography.
No differences were observed in age or body mass index among the groups, but blood pressures were higher in severe OSA compared with moderate and mild OSA. In severe OSA, the thickness of the IVS (11.6 [1.7 mm]), LVPW (10.7 [1.7 mm]), LVM (260.9 [50.5 g]), and LVMI (121.9 [21.1g/m2]) were higher than in moderate OSA (9.4 [1.3 mm]; 9.9 [1.6]; 196.4 [35.2]; 94.7 [13.2 g/m2], respectively) and mild OSA (9.8 [2.4 mm], 8.9 [2.0 mm], 187.6 [66.2 g], 95.8 [28.6 g/m2], respectively). In severe OSA, MPI (0.8 [0.2]) was significantly higher than in mild OSA (0.5 [P<.01]) but not significantly higher than moderate OSA (0.8 [0.1]).
OSA patients have demonstrable cardiac abnormalities that worsen with the severity of apnea. The MPI may have utility in subsequent OSA studies, possibly as a surrogate outcome measure.
阻塞性睡眠呼吸暂停(OSA)会导致心血管疾病的发病率和死亡率上升,包括系统性动脉高血压、冠心病、心律及传导紊乱、心力衰竭和中风。在我们的研究中,旨在评估OSA患者的左心室质量和心肌性能指数(MPI)。
2007年5月至2009年8月在土耳其伊斯坦布尔一家三级医院进行的一项横断面研究。
40名无任何心脏或肺部疾病的受试者因OSA评估接受了夜间多导睡眠图和超声心动图检查。根据呼吸暂停低通气指数(AHI),受试者被分为三组;轻度OSA(AHI:5 - 14次/小时;n = 7)、中度OSA(AHI:15 - 29次/小时;n = 13)和重度OSA(AHI:≥30次/小时;n = 20)。通过M型测量室间隔(IVS)和左心室后壁(LVPW)的厚度以及左心室质量(LVM)和LVM指数(LVMI)。通过多普勒超声心动图计算左心室MPI为(等容收缩时间 + 等容舒张时间)/主动脉射血时间。
各组间年龄或体重指数无差异,但重度OSA患者的血压高于中度和轻度OSA患者。在重度OSA中,IVS厚度(11.6 [1.7毫米])、LVPW厚度(10.7 [1.7毫米])、LVM(260.9 [50.5克])和LVMI(121.9 [21.1克/平方米])高于中度OSA(分别为9.4 [1.3毫米];9.9 [1.6];196.4 [35.2];94.7 [13.2克/平方米])和轻度OSA(分别为9.8 [2.4毫米],8.9 [2.0毫米],187.6 [66.2克],95.8 [28.6克/平方米])。在重度OSA中,MPI(0.8 [0.2])显著高于轻度OSA(0.5 [P <.01]),但不显著高于中度OSA(0.8 [0.1])。
OSA患者存在明显的心脏异常,且随着呼吸暂停严重程度加重而恶化。MPI可能在后续的OSA研究中有用,可能作为替代结局指标。