Kim Hye-Seon, Kim Ki-Bong, Hwang Ho Young, Chang Hyung Woo, Park Kyu-Joo
Department of Thoracic and Cardiovascular Surgery, Seoul National University Hospital, Seoul National University College of Medicine, Korea.
Korean J Thorac Cardiovasc Surg. 2012 Jun;45(3):161-5. doi: 10.5090/kjtcs.2012.45.3.161. Epub 2012 Jun 7.
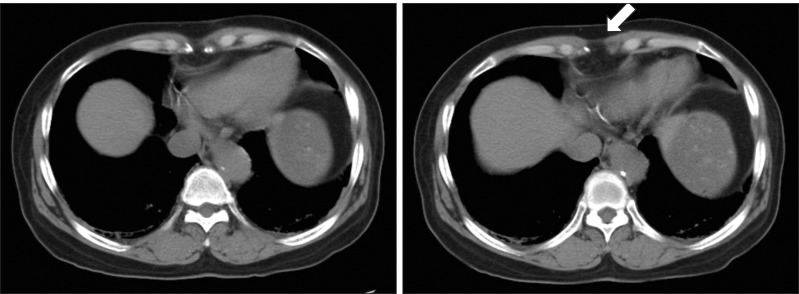
Median sternotomy can weaken the upper abdominal wall and result in subxiphoid incisional hernia. We evaluated risk factors associated with the development of subxiphoid incisional hernias after coronary artery bypass grafting (CABG).
Of 1,656 isolated CABGs performed between January 2001 and July 2010, 1,599 patients who were completely followed up were analyzed. The mean follow-up duration was 49.5±34.3 months. Subxiphoid incisional hernia requiring surgical repair developed in 13 patients (0.8%). The hernia was diagnosed 16.3±10.3 months postoperatively, and hernia repair was performed 25.0±26.1 months after the initial operation. Risk factors associated with the development of subxiphoid incisional hernia were analyzed with the Cox proportional hazard model.
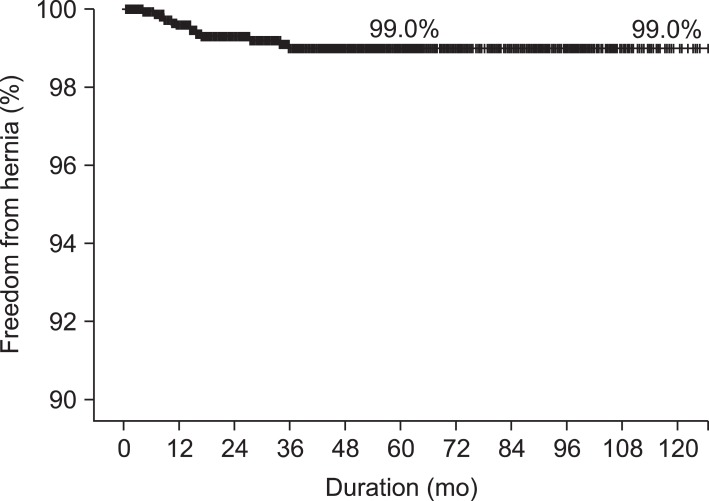
Five-year freedom from the hernia was 99.0%. Univariate analysis revealed that female sex (p=0.019), height (p=0.019), body surface area (p=0.046), redo operation (p=0.012), off-pump CABG (p=0.049), a postoperative wound problem (p=0.041), postoperative bleeding (p=0.046), and low cardiac output syndrome (p<0.001) were risk factors for the development of the hernia. Multivariable analysis showed that female sex (p=0.01) and low cardiac output syndrome (p<0.001) were associated with subxiphoid hernia formation.
Female sex and postoperative low cardiac output syndrome were risk factors of subxiphoid hernia. Therefore, special attention is needed for patients with high-risk factors.
正中胸骨切开术可削弱上腹壁并导致剑突下切口疝。我们评估了冠状动脉旁路移植术(CABG)后剑突下切口疝发生的相关危险因素。
对2001年1月至2010年7月期间进行的1656例单纯CABG手术患者中的1599例进行了完整随访分析。平均随访时间为49.5±34.3个月。13例患者(0.8%)发生了需要手术修复的剑突下切口疝。疝在术后16.3±10.3个月被诊断出来,疝修补术在初次手术后25.0±26.1个月进行。采用Cox比例风险模型分析与剑突下切口疝发生相关的危险因素。
5年无疝生存率为99.0%。单因素分析显示,女性(p=0.019)、身高(p=0.019)、体表面积(p=0.046)、再次手术(p=0.012)、非体外循环CABG(p=0.049)、术后伤口问题(p=0.041)、术后出血(p=0.046)和低心排血量综合征(p<0.001)是疝发生的危险因素。多因素分析表明,女性(p=0.01)和低心排血量综合征(p<0.001)与剑突下疝形成有关。
女性和术后低心排血量综合征是剑突下疝的危险因素。因此,对具有高危因素的患者需要特别关注。