Division of Hepatology, Montefiore Medical Center and Albert Einstein College of Medicine, 111 East 210th Street, Rosenthal 2 Red Zone, Bronx, NY 10467, USA.
Dig Dis Sci. 2012 Nov;57(11):2774-85. doi: 10.1007/s10620-012-2276-3. Epub 2012 Jun 26.
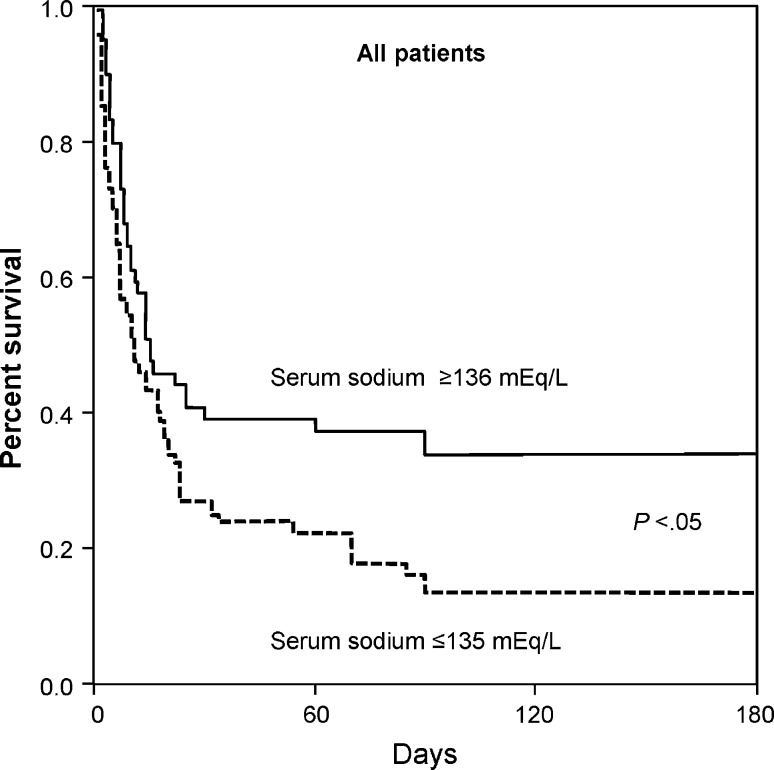
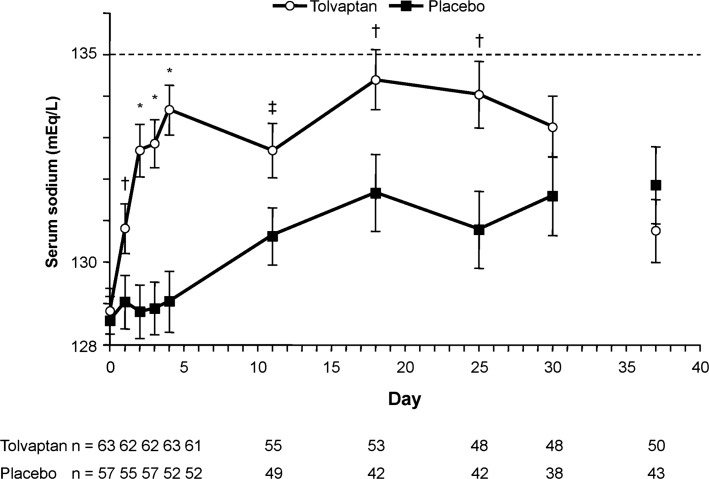
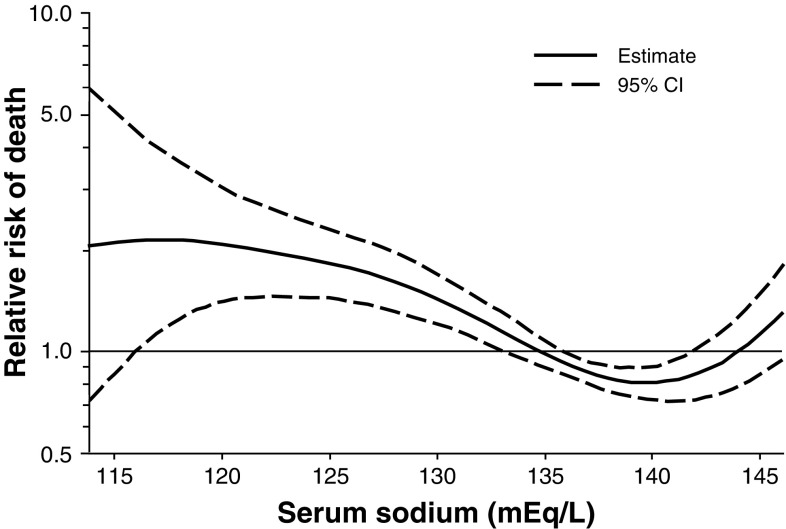
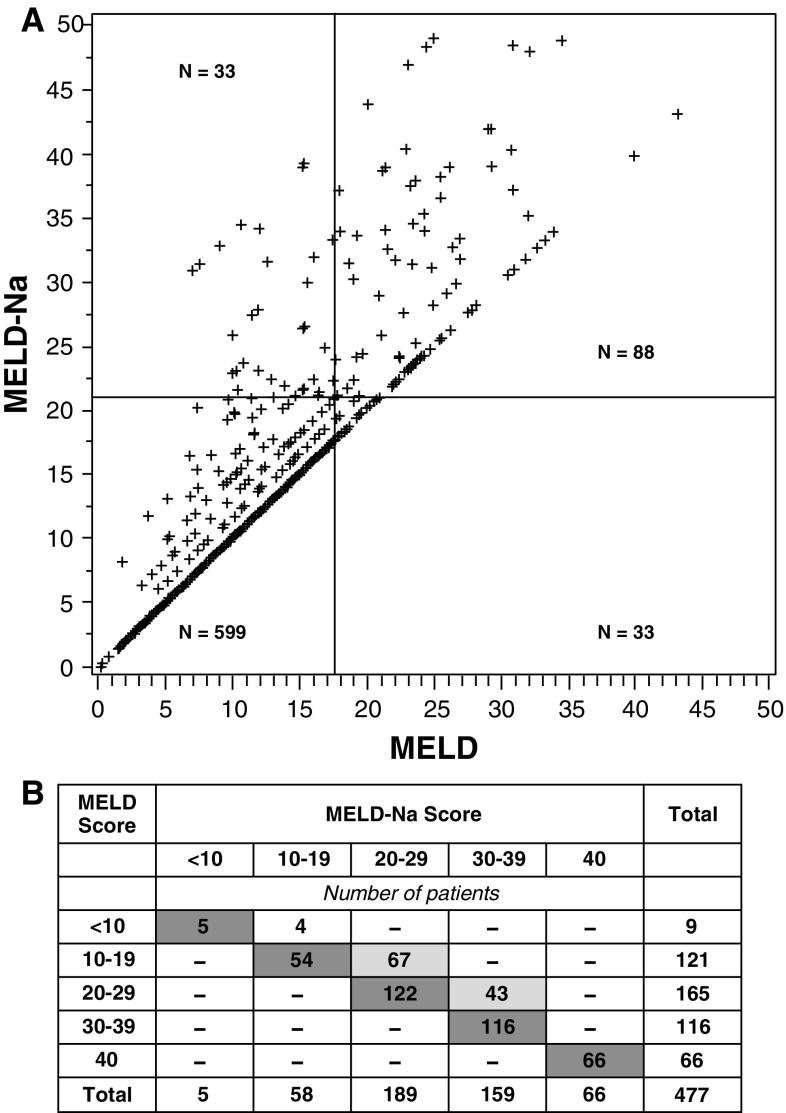
Hyponatremia is common in patients with cirrhosis and portal hypertension, and is characterized by excessive renal retention of water relative to sodium due to reduced solute-free water clearance. The primary cause is increased release of arginine vasopressin. Hyponatremia is associated with increased mortality in cirrhotic patients, those with end-stage liver disease (ESLD) on transplant waiting lists, and, in some studies, posttransplantation patients. Clinical evidence suggests that adding serum sodium to model for ESLD (MELD) scoring identifies patients in greatest need of liver transplantation by improving waiting list mortality prediction. Hyponatremia is also associated with numerous complications in liver disease patients, including severe ascites, hepatic encephalopathy, infectious complications, renal impairment, increased severity of liver disease in cirrhosis, and increased hospital stay and neurologic/infectious complications posttransplant. Vasopressin receptor antagonists, which act to increase free water excretion (aquaresis) and thereby increase serum sodium concentration, have been evaluated in patients with hypervolemic hyponatremia (including cirrhosis and heart failure) and euvolemic hyponatremia (SIADH). Tolvaptan, a selective vasopressin V(2)-receptor antagonist, is the only oral agent in this class approved for raising sodium levels in hypervolemic and euvolemic hyponatremia. The SALT trials showed that tolvaptan treatment rapidly and effectively resolved hyponatremia in these settings, including cirrhosis, and it has been shown that this agent can be safely and effectively used in long-term treatment. Fluid restriction should be avoided during the first 24 h of treatment to prevent overly rapid correction of hyponatremia, and tolvaptan should not be used in patients who cannot sense/respond to thirst, anuric patients, hypovolemic patients, and/or those requiring urgent intervention to raise serum sodium acutely.
低钠血症在肝硬化和门静脉高压患者中很常见,其特征是由于溶质自由水清除率降低,导致水相对于钠的肾脏潴留过多。主要原因是精氨酸血管加压素释放增加。低钠血症与肝硬化患者、终末期肝病(ESLD)患者在移植等待名单上的死亡率增加有关,并且在一些研究中,与移植后患者的死亡率增加有关。临床证据表明,通过向 ESLD 模型(MELD)评分添加血清钠来识别最需要肝移植的患者,可以提高等待名单的死亡率预测。低钠血症也与肝病患者的许多并发症有关,包括严重腹水、肝性脑病、感染性并发症、肾功能损害、肝硬化肝脏疾病严重程度增加,以及移植后住院时间延长和神经/感染性并发症增加。血管加压素受体拮抗剂可增加自由水排泄(aquaresis),从而增加血清钠浓度,已在高容量性低钠血症(包括肝硬化和心力衰竭)和等容量性低钠血症(SIADH)患者中进行了评估。托伐普坦是一种选择性血管加压素 V2-受体拮抗剂,是唯一批准用于升高高容量性和等容量性低钠血症患者血清钠水平的口服药物。SALT 试验表明,托伐普坦治疗可迅速有效地纠正这些情况下的低钠血症,包括肝硬化,并且已证明该药物可在长期治疗中安全有效地使用。在治疗的头 24 小时内应避免限制液体摄入,以防止低钠血症纠正过快,并应避免在不能感知/响应口渴、无尿患者、低血容量患者和/或需要紧急干预以快速提高血清钠的患者中使用托伐普坦。