Wilcox M Elizabeth, Adhikari Neill K J
Crit Care. 2012 Jul 18;16(4):R127. doi: 10.1186/cc11429.
Telemedicine extends intensivists' reach to critically ill patients cared for by other physicians. Our objective was to evaluate the impact of telemedicine on patients' outcomes.
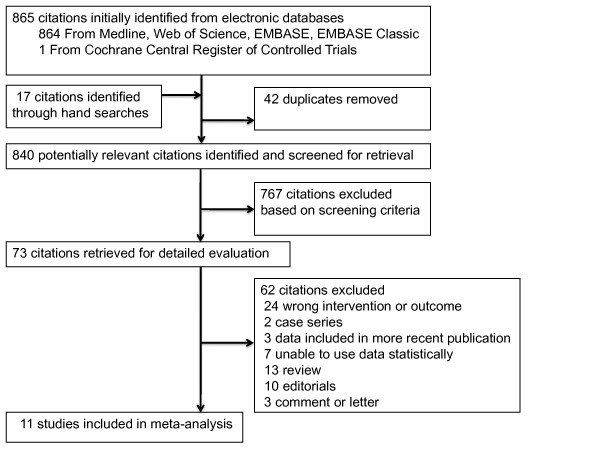
We searched electronic databases through April 2012, bibliographies of included trials, and indexes and conference proceedings in two journals (2001 to 2012). We selected controlled trials or observational studies of critically ill adults or children, examining the effects of telemedicine on mortality. Two authors independently selected studies and extracted data on outcomes (mortality and length of stay in the intensive care unit (ICU) and hospital) and methodologic quality. We used random-effects meta-analytic models unadjusted for case mix or cluster effects and quantified between-study heterogeneity by using I² (the percentage of total variability across studies attributable to heterogeneity rather than to chance).
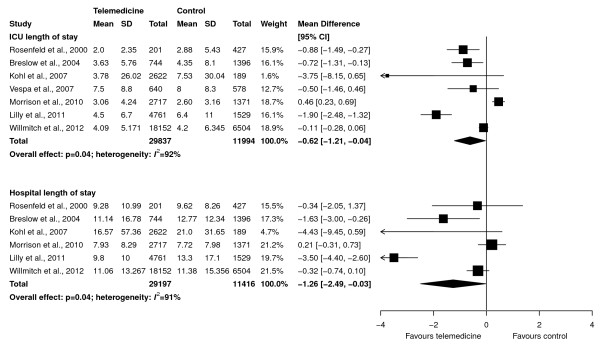
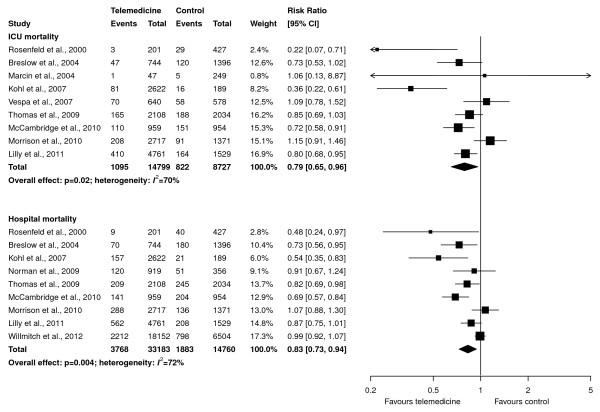
Of 865 citations, 11 observational studies met selection criteria. Overall quality was moderate (mean score on Newcastle-Ottawa scale, 5.1/9; range, 3 to 9). Meta-analyses showed that telemedicine, compared with standard care, is associated with lower ICU mortality (risk ratio (RR) 0.79; 95% confidence interval (CI), 0.65 to 0.96; nine studies, n = 23,526; I2 = 70%) and hospital mortality (RR, 0.83; 95% CI, 0.73 to 0.94; nine studies, n = 47,943; I² = 72%). Interventions with continuous patient-data monitoring, with or without alerts, reduced ICU mortality (RR, 0.78; 95% CI, 0.64 to 0.95; six studies, n = 21,384; I² = 74%) versus those with remote intensivist consultation only (RR, 0.64; 95% CI, 0.20 to 2.07; three studies, n = 2,142; I2 = 71%), but effects were statistically similar (interaction P = 0.74). Effects were also similar in higher (RR, 0.83; 95% CI, 0.68 to 1.02) versus lower (RR, 0.69; 95% CI, 0.40 to 1.19; interaction, P = 0.53) quality studies. Reductions in ICU and hospital length of stay were statistically significant (weighted mean difference (telemedicine-control), -0.62 days; 95% CI, -1.21 to -0.04 days and -1.26 days; 95% CI, -2.49 to -0.03 days, respectively; I2 > 90% for both).
Telemedicine was associated with lower ICU and hospital mortality among critically ill patients, although effects varied among studies and may be overestimated in nonrandomized designs. The optimal telemedicine technology configuration and dose tailored to ICU organization and case mix remain unclear.
远程医疗将重症监护医生的服务范围扩展到了由其他医生照料的危重症患者。我们的目标是评估远程医疗对患者预后的影响。
我们检索了截至2012年4月的电子数据库、纳入试验的参考文献以及两份期刊(2001年至2012年)的索引和会议论文集。我们选择了针对危重症成人或儿童的对照试验或观察性研究,以考察远程医疗对死亡率的影响。两位作者独立选择研究并提取有关预后(死亡率、重症监护病房(ICU)及住院时间)和方法学质量的数据。我们使用未针对病例组合或聚类效应进行调整的随机效应荟萃分析模型,并通过I²(各研究间总变异中归因于异质性而非机遇的百分比)对研究间异质性进行量化。
在865篇文献中,11项观察性研究符合入选标准。总体质量中等(纽卡斯尔 - 渥太华量表平均得分5.1/9;范围为3至9)。荟萃分析表明,与标准治疗相比,远程医疗与较低的ICU死亡率(风险比(RR)0.79;95%置信区间(CI),0.65至0.96;9项研究,n = 23,526;I² = 70%)和医院死亡率(RR,0.83;95%CI,0.73至0.94;9项研究,n = 47,943;I² = 72%)相关。采用连续患者数据监测(无论有无警报)的干预措施降低了ICU死亡率(RR,0.78;95%CI,0.64至0.95;6项研究,n = 21,384;I² = 74%),而仅采用远程重症监护医生会诊的干预措施降低ICU死亡率的效果为(RR,0.64;95%CI,0.20至2.07;3项研究,n = 2,142;I² = 71%),但效果在统计学上相似(交互作用P = 0.74)。在质量较高(RR,0.83;95%CI,0.68至1.02)和质量较低(RR,0.69;95%CI,0.40至1.19;交互作用,P = 0.53)的研究中效果也相似。ICU和医院住院时间的缩短具有统计学意义(加权平均差(远程医疗 - 对照),-0.62天;95%CI,-1.21至 -0.04天和 -1.26天;95%CI,-2.49至 -0.03天,两者I²均> 90%)。
远程医疗与危重症患者较低的ICU和医院死亡率相关,尽管各研究结果存在差异,且在非随机设计中可能被高估。针对ICU组织形式和病例组合的最佳远程医疗技术配置和剂量仍不明确。