Department of Pediatric Disciplines, North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences NEIGRIHMS, Mawdiangdiang, Shillong, Meghalaya, India.
Indian J Pediatr. 2013 May;80(5):359-64. doi: 10.1007/s12098-012-0855-0. Epub 2012 Jul 22.
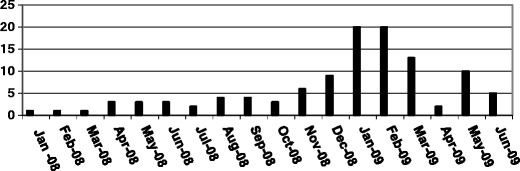
To report an outbreak of invasive meningococcal disease from Meghalaya, in the north east India, from January 2008 through June 2009.
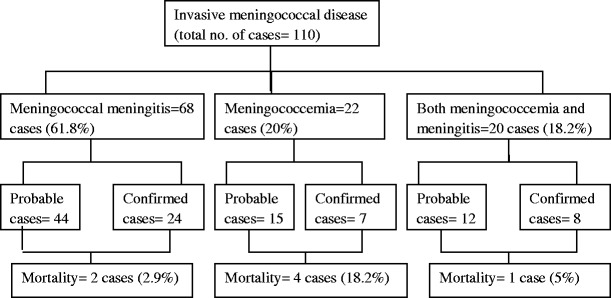
Retrospective review of case sheets was done. One hundred ten patients with invasive meningococcal disease were included for the study.
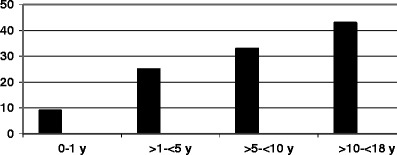
Of the total patients, 61.8 % were boys and 38.2 % were girls (boy to girl ratio = 1.62:1). The average age of presentation was 8.48 ± 5.09 y. Meningococcal meningitis was seen in 61.8 % of cases, meningococcemia in 20 % and 18.2 % had both. Fever was the most common manifestation (100 %) followed by meningeal signs (78.2 %), headache (56.4 %), vomiting (53.6 %), shock (38.2 %), low Glasgow coma scale (GCS) (25.5 %), purpura and rashes (23.6 %), seizures (9.1 %), abdominal symptoms (4.5 %), irritability and excessive crying (4.5 %) and bulging anterior fontanalle (23 %) in those below 18 mo of age. Raised intracranial pressure (ICP) was the most common complication (28.2 %) followed by coagulopathy (16.4 %), hepatopathy (10 %), herpes labialis (9.1 %), syndrome of inappropriate ADH secretion (SIADH) (8 %), pneumonia (7 %), arthritis (6 %), purpura fulminans, respiratory failure, sixth nerve palsy and diabetes insipidus in 4.5 % each, subdural empyema, optic neuritis, ARDS and ARF in 1.8 % each, cerebral salt wasting syndrome, third nerve palsy, cerebritis and hearing impairment in 0.9 % each. Culture was positive in 35.5 %. Patients were treated initially with ceftriaxone and dexamethasone but later on with chloramphenicol due to clinical drug resistance. Mortality was 6.4 %.
This is the first epidemic report of invasive meningococcal disease from the north east India. Chloramphenicol acts well in areas with penicillin or cephalosporin resistance. Mortality reduces significantly with early diagnosis and prompt intervention.
报告 2008 年 1 月至 2009 年 6 月印度东北部梅加拉亚邦发生的侵袭性脑膜炎奈瑟菌病疫情。
对病历进行回顾性分析。共有 110 例侵袭性脑膜炎奈瑟菌病患者纳入研究。
在所有患者中,61.8%为男性,38.2%为女性(男:女=1.62:1)。平均发病年龄为 8.48±5.09 岁。61.8%的病例为脑膜炎奈瑟菌性脑膜炎,20%为脑膜炎奈瑟菌血症,18.2%同时存在两种情况。发热是最常见的表现(100%),其次是脑膜刺激征(78.2%)、头痛(56.4%)、呕吐(53.6%)、休克(38.2%)、低格拉斯哥昏迷评分(GCS)(25.5%)、紫癜和皮疹(23.6%)、癫痫发作(9.1%)、腹部症状(4.5%)、烦躁不安和过度哭闹(4.5%)和 18 个月以下婴儿前囟隆起(23%)。颅内压升高(28.2%)是最常见的并发症,其次是凝血障碍(16.4%)、肝损害(10%)、唇疱疹(9.1%)、抗利尿激素分泌不当综合征(SIADH)(8%)、肺炎(7%)、关节炎(6%)、暴发性紫癜、呼吸衰竭、第六神经麻痹和尿崩症各 4.5%、硬膜下积脓、视神经炎、ARDS 和急性肾损伤各 1.8%、脑盐耗综合征、第三神经麻痹、脑脊髓炎和听力障碍各 0.9%。35.5%的病例培养阳性。患者最初接受头孢曲松和地塞米松治疗,但由于临床耐药性,后来改用氯霉素。死亡率为 6.4%。
这是印度东北部首次报告侵袭性脑膜炎奈瑟菌病疫情。氯霉素在青霉素或头孢菌素耐药地区效果良好。早期诊断和及时干预可显著降低死亡率。