Biomedical Department of Internal and Specialist Medicine, Section of Pulmonology, University of Palermo, Italy.
Int J Chron Obstruct Pulmon Dis. 2012;7:389-95. doi: 10.2147/COPD.S31630. Epub 2012 Jun 27.
The choice between lower limit of normal or fixed value of forced expiratory volume in one second/forced vital capacity ratio (FEV(1)/FVC) < 0.70 as the criterion for confirming airway obstruction is an open issue. In this study, we compared the criteria of lower limit of normal and fixed FEV(1)/FVC for diagnosis of airway obstruction, with a focus on healthy elderly people.
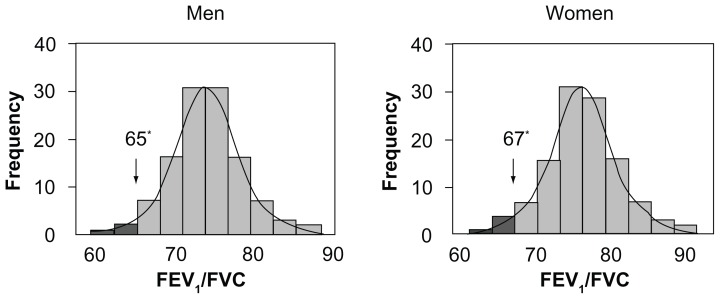
We selected 367 healthy nonsmoking subjects aged 65-93 years from 1971 participants in the population-based SARA (Salute Respiratoria nell'Anziano, Italian for "Respiratory Health in the Elderly") study, analyzed their spirometric data, and tested the relationship between spirometric indices and anthropometric variables. The lower limit of normal for FEV(1)/FVC was calculated as the fifth percentile of the normal distribution for selected subjects.
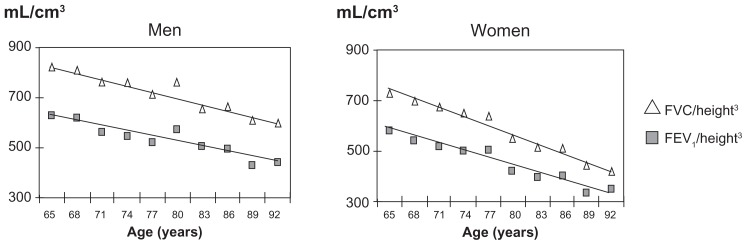
While FEV(1) and FVC decreased significantly with aging, the relationship between FEV(1)/FVC and age was not statistically significant in men or women. The lower limit of normal for FEV(1)/FVC was 0.65 in men and 0.67 in women. Fifty-five participants (15%) had FEV(1)/FVC < 0.70 and would have been inappropriately classified as obstructed according to the Global Initiative for Obstructive Lung Disease, American Thoracic Society/European Respiratory Society, and Canadian guidelines on chronic obstructive pulmonary disease. By applying different FEV(1)/FVC thresholds for the different age groups, as previously proposed in the literature, (0.70 for <70 years, 0.65 for 70-80 years, and 0.60 for >80 years) the percentage of patients classified as obstructed decreased to 6%. No subjects older than 80 years had an FEV(1)/FVC < 0.60.
The present results confirm the inadequacy of FEV(1)/FVC < 0.70 as a diagnostic criterion for airway obstruction after the age of 65 years. FEV(1)/FVC < 0.65 and <0.67 (for men and women, respectively) could identify subjects with airway obstruction in such a population. Further reduction of the threshold after 80 years is not justified.
在诊断气道阻塞时,选择使用正常下限值或一秒用力呼气量/用力肺活量比值(FEV1/FVC)<0.70 作为标准仍然存在争议。本研究比较了正常下限值和固定 FEV1/FVC 作为诊断气道阻塞的标准,重点关注健康的老年人。
我们从基于人群的 SARA(意大利语“Respiratoria nell'Anziano”,意为“老年人的呼吸健康”)研究的 1971 名参与者中选择了 367 名 65-93 岁的非吸烟健康受试者,分析他们的肺活量测定数据,并测试肺活量测定指数与人体测量学变量之间的关系。FEV1/FVC 的正常下限值是通过对选定的受试者进行正态分布的第 5 个百分位数计算得出的。
虽然 FEV1 和 FVC 随年龄增长而显著下降,但男性或女性的 FEV1/FVC 与年龄之间的关系没有统计学意义。FEV1/FVC 的正常下限值在男性中为 0.65,在女性中为 0.67。55 名(15%)参与者的 FEV1/FVC<0.70,根据全球慢性阻塞性肺疾病倡议、美国胸科学会/欧洲呼吸学会和加拿大慢性阻塞性肺疾病指南,他们将被不恰当地归类为阻塞性。通过应用文献中提出的不同年龄组的不同 FEV1/FVC 阈值(<70 岁为 0.70,70-80 岁为 0.65,>80 岁为 0.60),被归类为阻塞性的患者比例降至 6%。没有 80 岁以上的受试者的 FEV1/FVC<0.60。
本研究结果证实,65 岁以上人群中,FEV1/FVC<0.70 不能作为诊断气道阻塞的标准。在该人群中,FEV1/FVC<0.65 和<0.67(分别适用于男性和女性)可以识别气道阻塞的受试者。80 岁以后进一步降低阈值没有依据。