Johansson Silvia, Aström Lennart, Sandin Fredrik, Isacsson Ulf, Montelius Anders, Turesson Ingela
Section of Oncology, Department of Radiology, Oncology and Radiation Science, Uppsala University Hospital, 751 85 Uppsala, Sweden.
Prostate Cancer. 2012;2012:654861. doi: 10.1155/2012/654861. Epub 2012 Jul 8.
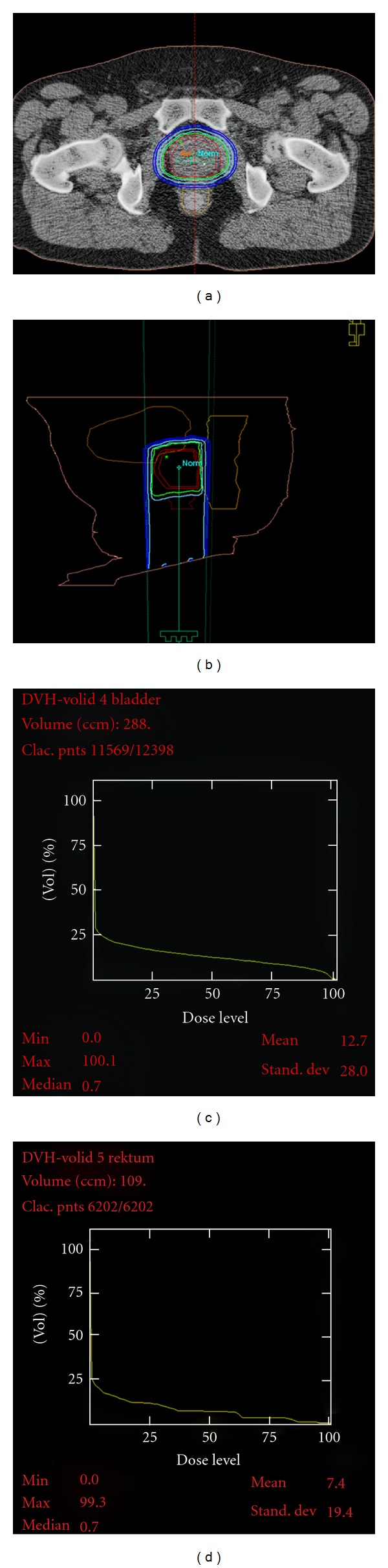
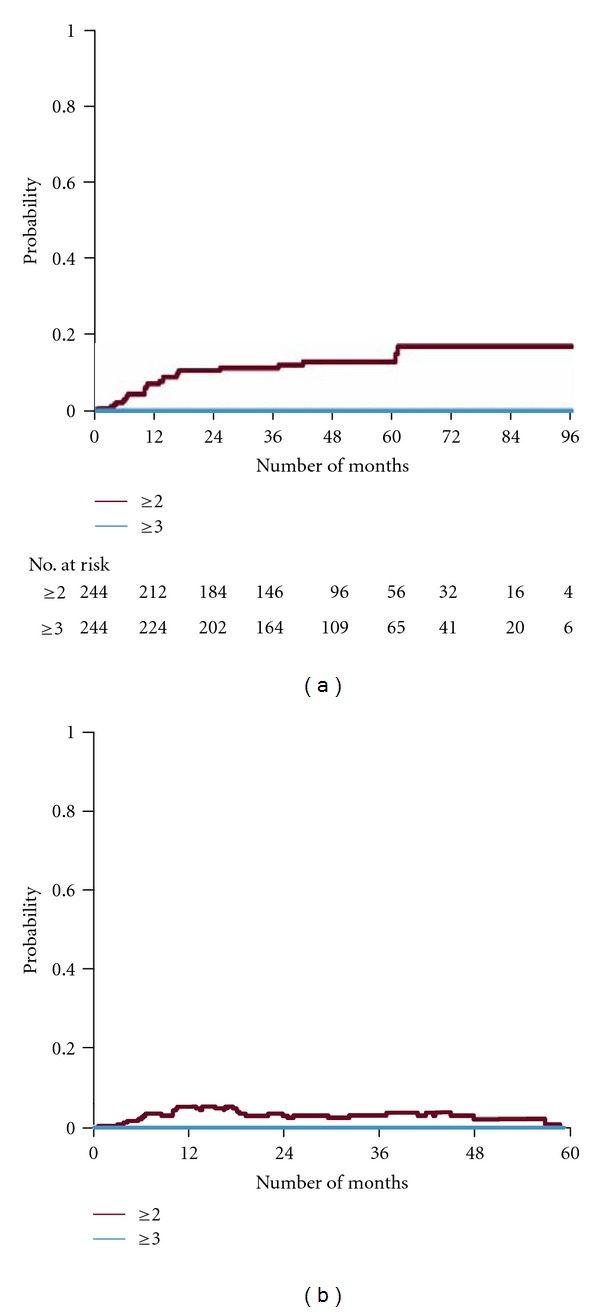
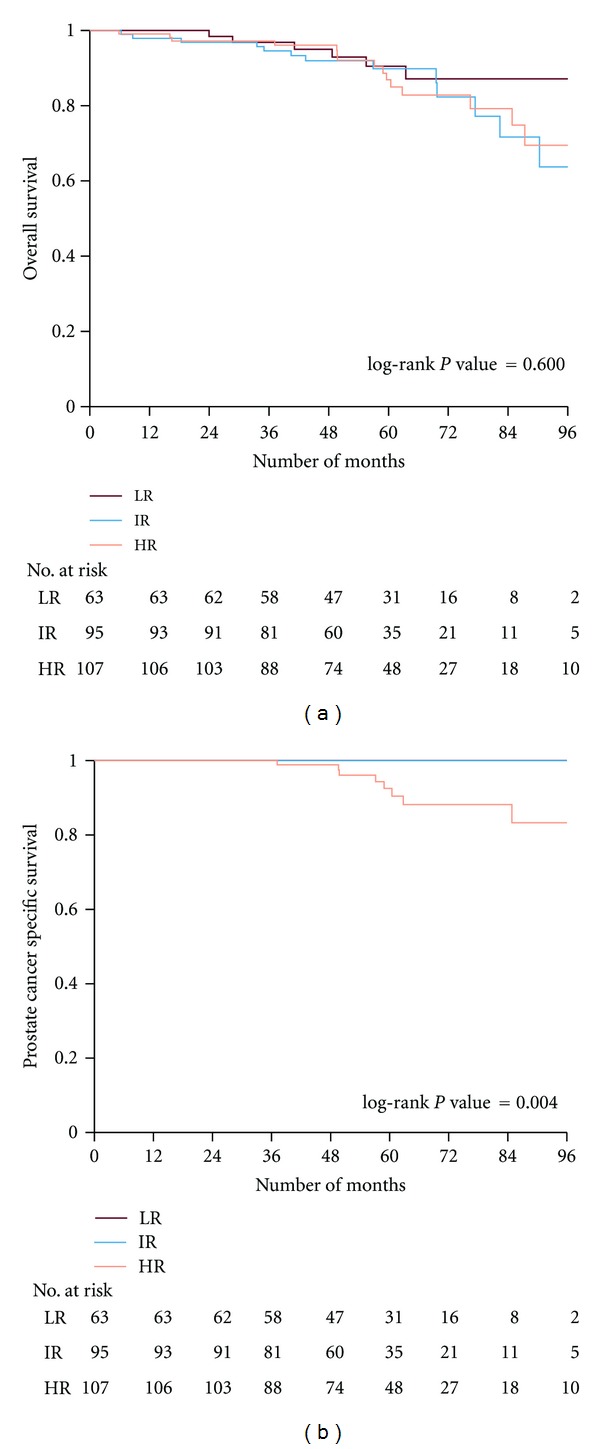
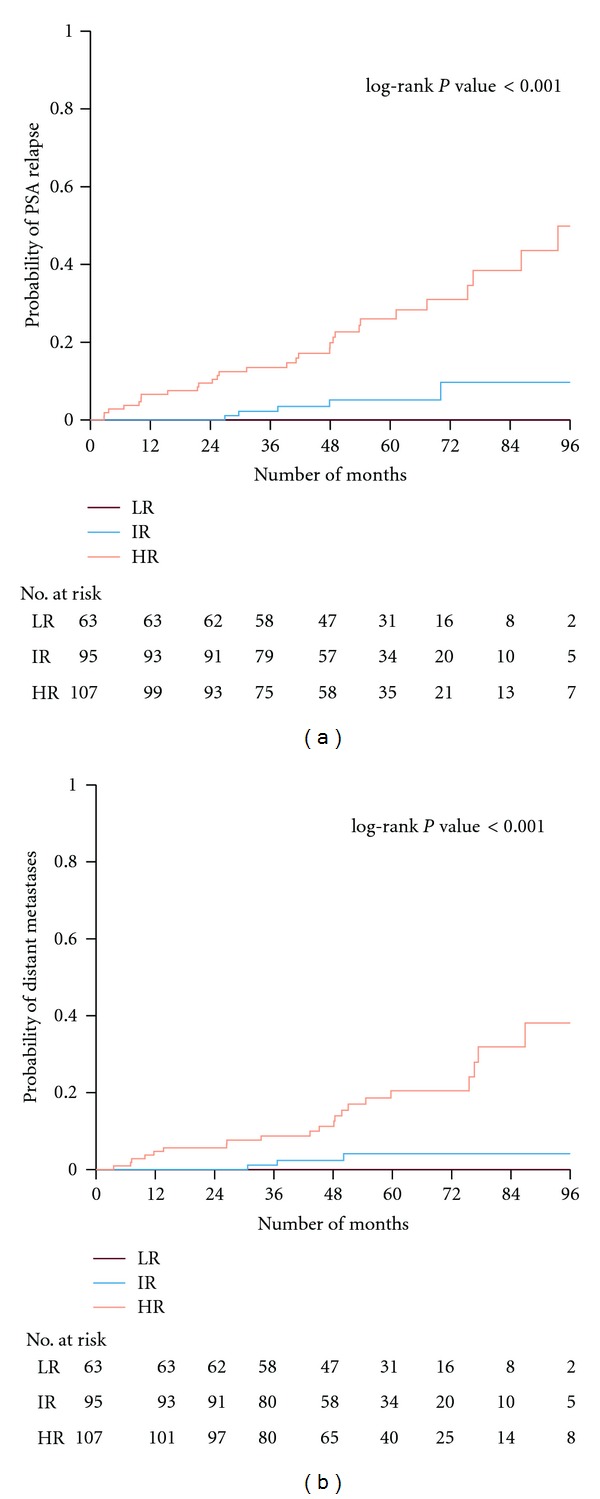
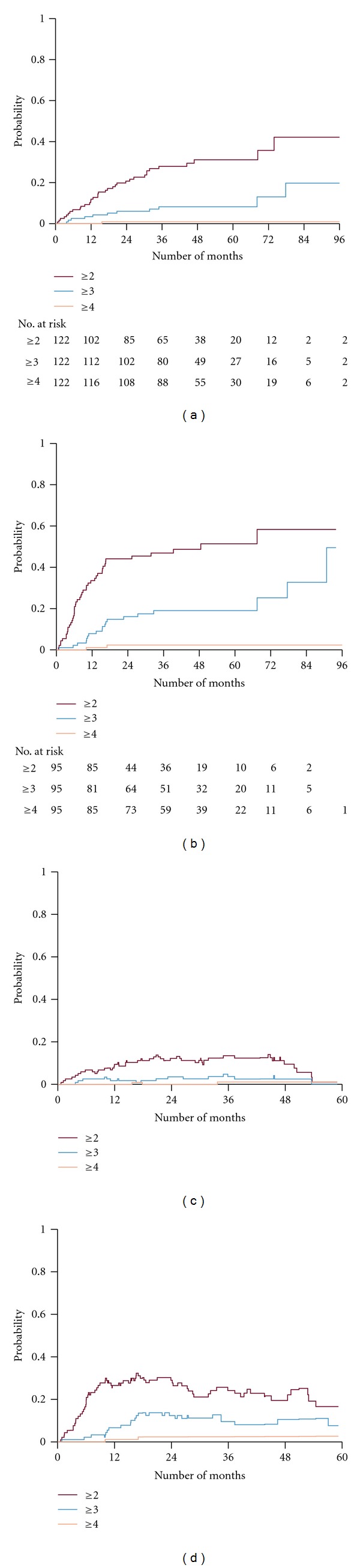
Proton boost of 20 Gy in daily 5 Gy fractions followed by external beam radiotherapy (EBRT) of 50 Gy in daily 2 Gy fractions were given to 278 patients with prostate cancer with T1b to T4N0M0 disease. Fifty-three percent of the patients received neoadjuvant androgen deprivation therapy (N-ADT). The medium followup was 57 months. The 5-year PSA progression-free survival was 100%, 95%, and 74% for low-, intermediate-, and high-risk patients, respectively. The toxicity evaluation was supported by a patient-reported questionnaire before every consultant visit. Cumulative probability and actuarial prevalence of genitourinary (GU) and gastrointestinal (GI) toxicities are presented according to the RTOG classification. N-ADT did not influence curability. Mild pretreatment GU-symptoms were found to be a strong predictive factor for GU-toxicity attributable to treatment. The actuarial prevalence declined over 3 to 5 years for both GU and GI toxicities, indicating slow resolution of epithelial damage to the genitourinary and gastrointestinal tract. Bladder toxicities rather than gastrointestinal toxicities seem to be dose limiting. More than 5-year followup is necessary to reveal any sign of true progressive late side effects of the given treatment. Hypofractionated proton-boost combined with EBRT is associated with excellent curability of localized PC and acceptable frequencies of treatment toxicity.
278例T1b至T4N0M0期前列腺癌患者接受了每日5Gy分次共20Gy的质子增敏治疗,随后接受每日2Gy分次共50Gy的外照射放疗(EBRT)。53%的患者接受了新辅助雄激素剥夺治疗(N-ADT)。中位随访时间为57个月。低、中、高危患者的5年无前列腺特异性抗原(PSA)进展生存率分别为100%、95%和74%。在每次会诊前通过患者报告问卷进行毒性评估。根据美国放射肿瘤学协作组(RTOG)分类给出泌尿生殖系统(GU)和胃肠道(GI)毒性的累积概率和精算患病率。N-ADT不影响治愈率。发现轻度治疗前GU症状是治疗所致GU毒性的强预测因素。GU和GI毒性的精算患病率在3至5年内均下降,表明泌尿生殖道和胃肠道上皮损伤的缓解缓慢。膀胱毒性而非胃肠道毒性似乎是剂量限制因素。需要超过5年的随访来揭示给定治疗真正进行性晚期副作用的任何迹象。大分割质子增敏联合EBRT与局限性前列腺癌的优异治愈率和可接受的治疗毒性发生率相关。