World Health Organisation, Malawi Country Office, Lilongwe, Malawi.
BMC Int Health Hum Rights. 2012 Aug 6;12:12. doi: 10.1186/1472-698X-12-12.
Although leprosy was eliminated globally in 2000, the disease continues to be the significant cause of peripheral neuropathy, disability and disfigurement in some developing countries. However, recent population-based prevalence data are lacking to inform evidence-based renewed commitment for the final push for leprosy elimination at national and sub-national levels.
Community camp-based cross-sectional descriptive study was conducted in four selected districts. World Health Organisation guidelines and tools for leprosy elimination monitoring were used to evaluate the Malawi National Leprosy Programme.
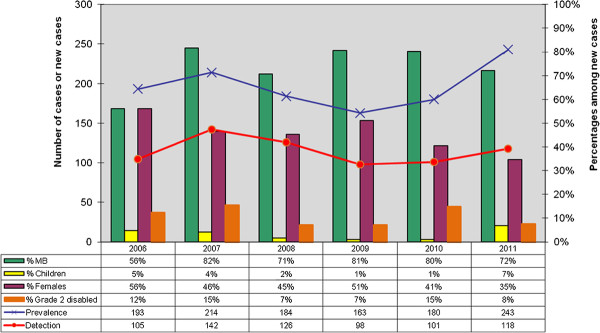
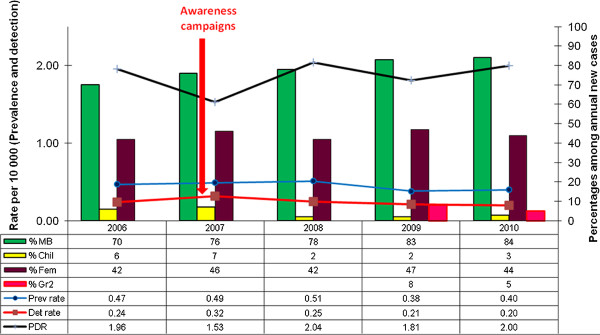
A total of 6,338 people (60% females, 35% children aged less than 15 years) were examined for leprosy and other skin diseases. Prevalence of skin diseases was 18%, the commonest being fungal (9%), eczema/dermatitis (3%) and leprosy (1%). Of the fungal skin conditions, pityriasis versicolor and Tinea capatis were the commonest (22% and 21% respectively) then Tinea corporis (9%), Tinea cruris (6%) and Tinea pedis (2%). A total of 66 leprosy cases were detected out of 6,338 people screened giving a prevalence of 104.1 per 10,000 population (range by district 67.1 to 194.1). Of the leprosy cases, 37 were new, 6 were defaulters and 23 were on treatment, 30 were females and 9 were children aged less than 15 years old. Of the 37 new leprosy cases, 9 (24.3%) were children, 25 (67.6%) had 1-5 leprosy lesions and 8 (21.6%) had grade 2 disability. The most frequent location of leprosy lesions was the head and neck (24.1%), arms (24.1%), chest (17.2%), legs (13.8%), back (13.8%) and abdomen (7.0%). Between 2006 and 2011, trends of leprosy prevalence and detection increased, prevalence/detection ratios were over 1 and cure rates by cohort analysis of 2009 multibacillary and 2010 paucibacillary cases were 33% and 63% respectively far below the expected 80% although the national prevalence remained at less than 1 case per 10,000 population.
Leprosy was still an important public health problem in Malawi. Improving knowledge and skills of health workers, registration and recording of data, contact tracing, decentralisation and integration of treatment to health centres and introduction of leprosy awareness days and community-based surveillance could help to improve early detection, treatment, case holding and prevention of disabilities.
尽管 2000 年全球已消灭麻风病,但该病在一些发展中国家仍是导致周围神经病变、残疾和毁容的主要原因。然而,目前缺乏基于人群的患病率数据,无法为国家和国家以下各级最后推动消灭麻风病提供循证的新承诺。
在四个选定的地区进行了以社区营地为基础的横断面描述性研究。采用世界卫生组织消除麻风病监测指南和工具评估马拉维国家麻风病规划。
共有 6338 人(60%为女性,35%为年龄小于 15 岁的儿童)接受了麻风病和其他皮肤病的检查。皮肤病患病率为 18%,最常见的是真菌感染(9%)、湿疹/皮炎(3%)和麻风病(1%)。在真菌感染性皮肤病中,花斑癣和头癣最为常见(分别为 22%和 21%),其次是体癣(9%)、股癣(6%)和足癣(2%)。在筛查的 6338 人中发现了 66 例麻风病病例,患病率为每 10000 人 104.1 例(按地区计算,患病率范围为 67.1 至 194.1)。在这些麻风病病例中,37 例为新病例,6 例为失访病例,23 例正在治疗中,30 例为女性,9 例为年龄小于 15 岁的儿童。在 37 例新的麻风病病例中,9 例(24.3%)为儿童,25 例(67.6%)有 1-5 个麻风病损伤,8 例(21.6%)有 2 级残疾。麻风病损伤最常见的部位是头部和颈部(24.1%)、手臂(24.1%)、胸部(17.2%)、腿部(13.8%)、背部(13.8%)和腹部(7.0%)。2006 年至 2011 年期间,麻风病的患病率和检出率呈上升趋势,患病率/检出率比值超过 1,2009 年多菌型和 2010 年少菌型病例的治愈率通过队列分析分别为 33%和 63%,远低于预期的 80%,尽管全国的患病率仍低于每 10000 人 1 例。
麻风病在马拉维仍是一个重要的公共卫生问题。提高卫生工作者的知识和技能、登记和记录数据、接触者追踪、权力下放和将治疗纳入卫生中心、引入麻风病宣传日以及开展社区监测,有助于提高早期发现、治疗、病例管理和预防残疾的能力。