Departments of Radiation Oncology, Surgery and Biostatistics, University of Toronto and Ontario Cancer Institute/Princess Margaret Hospital (University Health Network), Toronto, Ontario, Canada.
Br J Cancer. 2012 Aug 21;107(5):840-6. doi: 10.1038/bjc.2012.345. Epub 2012 Aug 7.
High plasma osteopontin (OPN) has been linked to tumour hypoxia, metastasis, and poor prognosis. This study aims to assess whether plasma osteopontin was a biomarker of increasing progression within prostate cancer (PCa) prognostic groups and whether it reflected treatment response to local and systemic therapies.
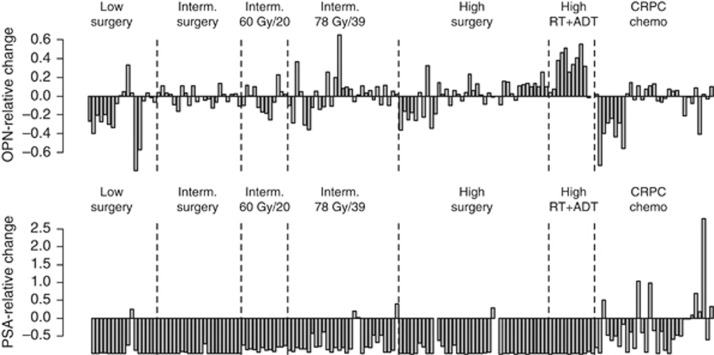
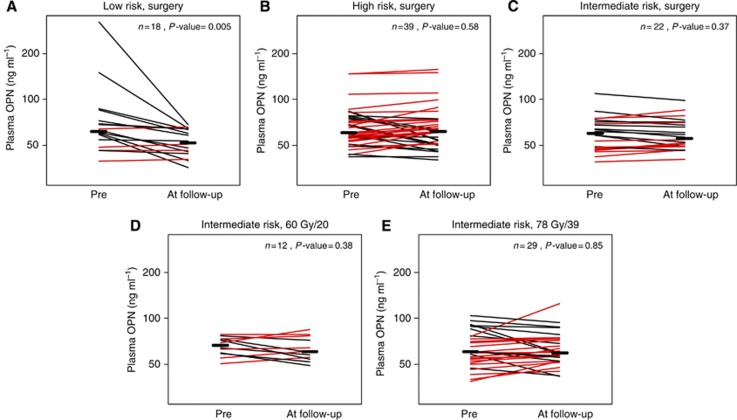
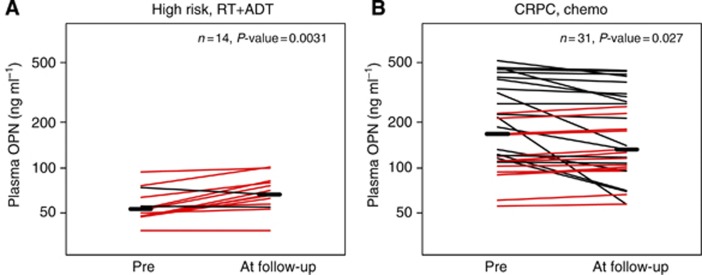
Baseline OPN was determined in men with localised (n=199), locally recurrent (n=9) and castrate-resistant, metastatic PCa (CRPC-MET; n=37). Receiver-operating curves (ROC) were generated to describe the accuracy of OPN for distinguishing between localised risk groups or localised vs metastatic disease. We also measured OPN pre- and posttreatment, following radical prostatectomy, external beam radiotherapy (EBRT), androgen deprivation (AD) or taxane-based chemotherapy.
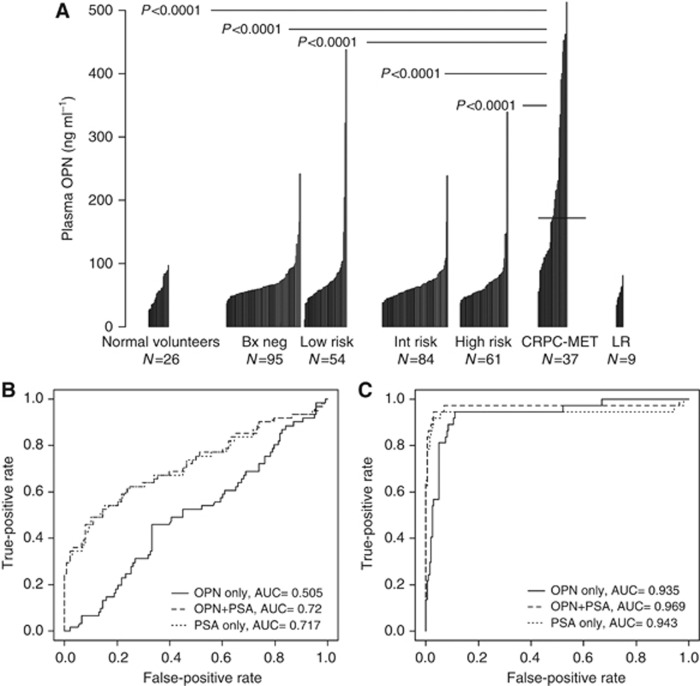
The CRPC-MET patients had increased baseline values (mean 219; 56-513 ng ml(-1); P<0.0001) compared with the localised, non-metastatic group (mean 72; 12-438 ng ml(-1)). The area under the ROC to differentiate localised vs metastatic disease was improved when OPN was added to prostate-specific antigen (PSA) (0.943-0.969). Osteopontin neither distinguished high-risk PCa from other localised PCa nor correlated with serum PSA at baseline. Osteopontin levels reduced in low-risk patients after radical prostatectomy (P=0.005) and in CRPC-MET patients after chemotherapy (P=0.027), but not after EBRT or AD.
Plasma OPN is as good as PSA at predicting treatment response in CRPC-MET patients after chemotherapy. Our data do not support the use of plasma OPN as a biomarker of increasing tumour burden within localised PCa.
高血浆骨桥蛋白(OPN)与肿瘤缺氧、转移和预后不良有关。本研究旨在评估血浆骨桥蛋白是否是前列腺癌(PCa)预后分组中进展程度的生物标志物,以及它是否反映了局部和全身治疗的反应。
在局部(n=199)、局部复发(n=9)和去势抵抗性转移性前列腺癌(CRPC-MET;n=37)患者中测定基线 OPN。生成接收者操作曲线(ROC)来描述 OPN 区分局部风险组或局部与转移性疾病的准确性。我们还在根治性前列腺切除术、外照射放疗(EBRT)、雄激素剥夺(AD)或紫杉烷类化疗后测量了 OPN 治疗前后的值。
CRPC-MET 患者的基线值(平均值 219;56-513ng/ml;P<0.0001)高于局部非转移性组(平均值 72;12-438ng/ml)。当 OPN 与前列腺特异性抗原(PSA)联合使用时,ROC 区分局部与转移性疾病的曲线下面积得到改善(0.943-0.969)。OPN 既不能区分高危 PCa 与其他局部 PCa,也不能与基线时的血清 PSA 相关。在根治性前列腺切除术后,低危患者的 OPN 水平降低(P=0.005),在化疗后 CRPC-MET 患者的 OPN 水平降低(P=0.027),但 EBRT 或 AD 后则没有降低。
在化疗后 CRPC-MET 患者中,血浆 OPN 与 PSA 一样能预测治疗反应。我们的数据不支持将血浆 OPN 用作局部 PCa 肿瘤负荷增加的生物标志物。