Department of Internal Medicine (Divisions of Cardiology, Hepatology, Geriatrics, and Integrated Medicine), Nippon Medical School, Tokyo, Japan.
Cardiovasc Diabetol. 2012 Aug 14;11:98. doi: 10.1186/1475-2840-11-98.
Previous studies have demonstrated that postprandial hyperglycemia attenuates brachial artery flow-mediated dilation (FMD) in prediabetic patients, in diabetic patients, and even in normal subjects. We have previously reported that postprandial hyperinsulinemia also attenuates FMD. In the present study we evaluated the relationship between different degrees of postprandial attenuation of FMD induced by postprandial hyperglycemia and hyperinsulinemia and differences in ingested carbohydrate content in non-diabetic individuals.
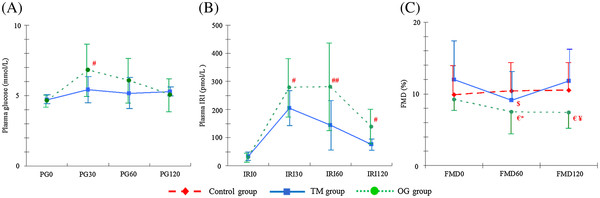
Thirty-seven healthy subjects with no family history of diabetes were divided into 3 groups: a 75-g oral glucose loading group (OG group) (n = 14), a test meal group (TM group) (n = 12; 400 kcal, carbohydrate content 40.7 g), and a control group (n = 11). The FMD was measured at preload (FMD0) and at 60 minutes (FMD60) and 120 (FMD120) minutes after loading. Plasma glucose (PG) and immunoreactive insulin (IRI) levels were determined at preload (PG0, IRI0) and at 30 (PG30, IRI30), 60 (PG60, IRI60), and 120 (PG120, IRI120) minutes after loading.
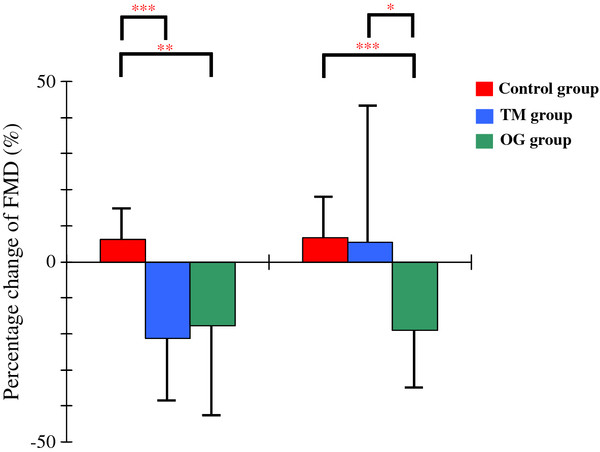
Percentage decreases from FMD0 to FMD60 were significantly greater in the TM group (-21.19% ± 17.90%; P < 0.001) and the OG group (-17.59% ± 26.64%) than in the control group (6.46% ± 9.17%; P < 0.01), whereas no significant difference was observed between the TM and OG groups. In contrast, the percentage decrease from FMD0 to FMD120 was significantly greater in the OG group (-18.91% ± 16.58%) than in the control group (6.78% ± 11.43%; P < 0.001) or the TM group (5.22% ± 37.22%; P < 0.05), but no significant difference was observed between the control and TM groups. The FMD60 was significantly correlated with HOMA-IR (r = -0.389; P < 0.05). In contrast, FMD120 was significantly correlated with IRI60 (r = -0.462; P < 0.05) and the AUC of IRI (r = -0.468; P < 0.05). Furthermore, the percentage change from FMD0 to FMD120 was significantly correlated with the CV of PG (r = 0.404; P < 0.05), IRI60 (r = 0.401; p < 0.05) and the AUC of IRI (r = 0.427; P < 0.05). No significant correlation was observed between any other FMDs and glucose metabolic variables.
Differences in the attenuation of postprandial FMD induced by different postprandial insulin levels may occur a long time postprandially but not shortly after a meal.
先前的研究已经证明,在糖尿病前期患者、糖尿病患者甚至在正常人群中,餐后高血糖会减弱肱动脉血流介导的扩张(FMD)。我们之前曾报道过,餐后高胰岛素血症也会减弱 FMD。在本研究中,我们评估了餐后高血糖和高胰岛素血症诱导的 FMD 不同程度的餐后衰减与非糖尿病个体摄入的碳水化合物含量之间的关系。
将 37 名无糖尿病家族史的健康受试者分为 3 组:75g 口服葡萄糖负荷组(OG 组)(n = 14)、试验餐组(TM 组)(n = 12;400kcal,碳水化合物含量 40.7g)和对照组(n = 11)。在负荷前(FMD0)和负荷后 60 分钟(FMD60)和 120 分钟(FMD120)测量 FMD。在负荷前(PG0、IRI0)和负荷后 30 分钟(PG30、IRI30)、60 分钟(PG60、IRI60)和 120 分钟(PG120、IRI120)测定血浆葡萄糖(PG)和免疫反应性胰岛素(IRI)水平。
TM 组(-21.19%±17.90%;P<0.001)和 OG 组(-17.59%±26.64%)与对照组(6.46%±9.17%;P<0.01)相比,从 FMD0 到 FMD60 的百分比下降明显更大,而 TM 组和 OG 组之间无显著差异。相比之下,OG 组(-18.91%±16.58%)与对照组(6.78%±11.43%;P<0.001)或 TM 组(5.22%±37.22%;P<0.05)相比,从 FMD0 到 FMD120 的百分比下降明显更大,但对照组和 TM 组之间无显著差异。FMD60 与 HOMA-IR 呈显著负相关(r = -0.389;P<0.05)。相反,FMD120 与 IRI60 呈显著负相关(r = -0.462;P<0.05)和 IRI 的 AUC 呈显著负相关(r = -0.468;P<0.05)。此外,从 FMD0 到 FMD120 的百分比变化与 PG 的 CV(r = 0.404;P<0.05)、IRI60(r = 0.401;P<0.05)和 IRI 的 AUC(r = 0.427;P<0.05)呈显著正相关。其它任何 FMD 与葡萄糖代谢变量之间均无显著相关性。
不同餐后胰岛素水平引起的餐后 FMD 减弱可能在餐后很长时间内发生,而不是在餐后不久。