University of Western Ontario, London, ON, Canada.
Int J Qual Health Care. 2012 Oct;24(5):538-46. doi: 10.1093/intqhc/mzs043. Epub 2012 Aug 14.
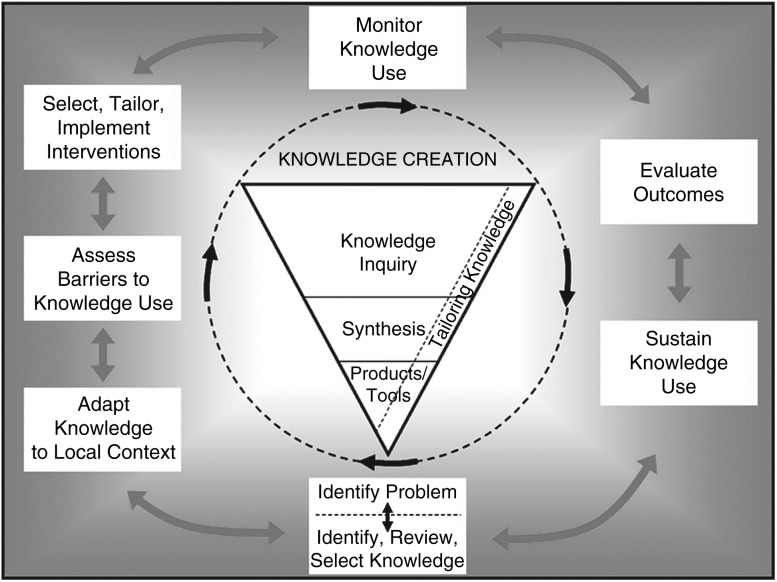
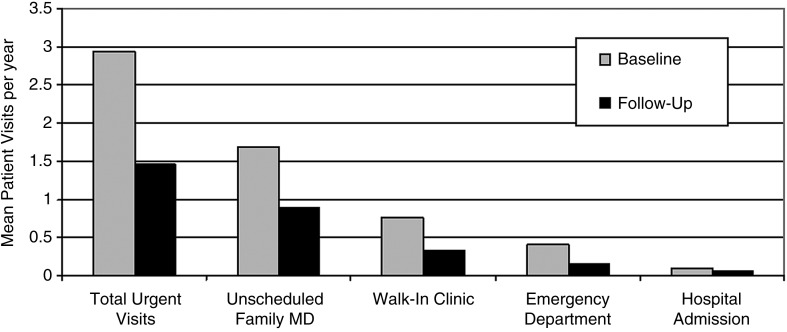
Quality problem International guidelines establish evidence-based standards for asthma care; however, recommendations are often not implemented and many patients do not meet control targets. Initial assessment Regional pilot data demonstrated a knowledge-to-practice gap. Choice of solutions We engineered health system change in a multi-step approach described by the Canadian Institutes of Health Research knowledge translation framework. Implementation Knowledge translation occurred at multiple levels: patient, practice and local health system. A regional administrative infrastructure and inter-disciplinary care teams were developed. The key project deliverable was a guideline-based interdisciplinary asthma management program. Six community organizations, 33 primary care physicians and 519 patients participated. The program operating cost was $290/patient. Evaluation Six guideline-based care elements were implemented, including spirometry measurement, asthma controller therapy, a written self-management action plan and general asthma education, including the inhaler device technique, role of medications and environmental control strategies in 93, 95, 86, 100, 97 and 87% of patients, respectively. Of the total patients 66% were adults, 61% were female, the mean age was 35.7 (SD = ± 24.2) years. At baseline 42% had two or more symptoms beyond acceptable limits vs. 17% (P< 0.001) post-intervention; 71% reported urgent/emergent healthcare visits at baseline (2.94 visits/year) vs. 45% (1.45 visits/year) (P< 0.001); 39% reported absenteeism (5.0 days/year) vs. 19% (3.0 days/year) (P< 0.001). The mean follow-up interval was 22 (SD = ± 7) months. Lessons learned A knowledge-translation framework can guide multi-level organizational change, facilitate asthma guideline implementation, and improve health outcomes in community primary care practices. Program costs are similar to those of diabetes programs. Program savings offset costs in a ratio of 2.1:1.
质量问题
国际指南为哮喘护理制定了基于证据的标准;然而,建议往往没有得到实施,许多患者也未达到控制目标。
初始评估
区域试点数据显示出知识与实践之间的差距。
解决方案选择
我们采用加拿大卫生研究院知识转化框架中描述的多步骤方法来改变卫生系统。
知识转化
患者、实践和当地卫生系统。建立了区域行政基础设施和跨学科护理团队。该项目的主要交付成果是基于指南的跨学科哮喘管理方案。有 6 个社区组织、33 名初级保健医生和 519 名患者参与了该方案。该方案的运营成本为每位患者 290 美元。
评估
实施了 6 项基于指南的护理要素,包括肺活量测量、哮喘控制药物治疗、书面自我管理行动计划以及一般哮喘教育,包括吸入器装置技术、药物作用和环境控制策略,分别在 93%、95%、86%、100%、97%和 87%的患者中得到应用。在所有患者中,66%为成年人,61%为女性,平均年龄为 35.7 岁(标准差=±24.2)。在基线时,42%的患者有两个或更多超出可接受范围的症状,而干预后这一比例为 17%(P<0.001);71%的患者在基线时有紧急/紧急医疗就诊,而干预后这一比例为 45%(P<0.001);39%的患者报告缺勤(每年 5.0 天),而干预后这一比例为 19%(每年 3.0 天)(P<0.001)。平均随访间隔为 22 个月(标准差=±7)。
经验教训
知识转化框架可以指导多层次的组织变革,促进哮喘指南的实施,并改善社区初级保健实践中的健康结果。方案成本与糖尿病方案相似。方案节省的费用可以抵消成本,比例为 2.1:1。