Department of Internal Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
Clin Mol Hepatol. 2012 Jun;18(2):185-94. doi: 10.3350/cmh.2012.18.2.185. Epub 2012 Jun 26.
BACKGROUND/AIMS: We compared the accuracy and usefulness of clinical diagnostic criteria for hepatocellular carcinoma in a hepatitis B virus (HBV)-endemic area.
We reviewed the medical records of 355 patients who had undergone liver resection or biopsy at our institution between January 2008 and December 2009. These patients were reevaluated using four noninvasive diagnostic criteria for hepatocellular carcinoma proposed by the European Association for the Study of the Liver (EASL), the American Association for the Study of Liver Diseases (AASLD), the Korean Liver Cancer Study Group and the National Cancer Center (KLCSG/NCC), and National Comprehensive Cancer Network (NCCN) guidelines.
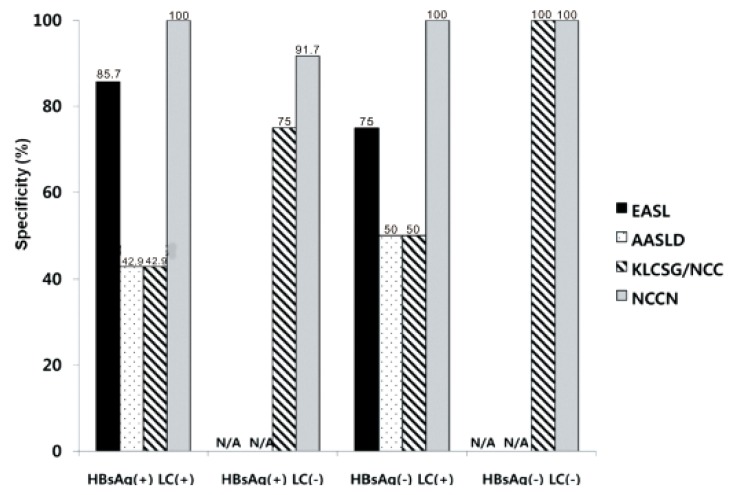
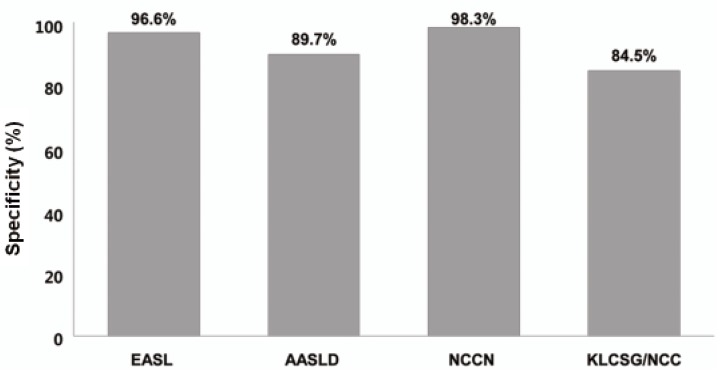
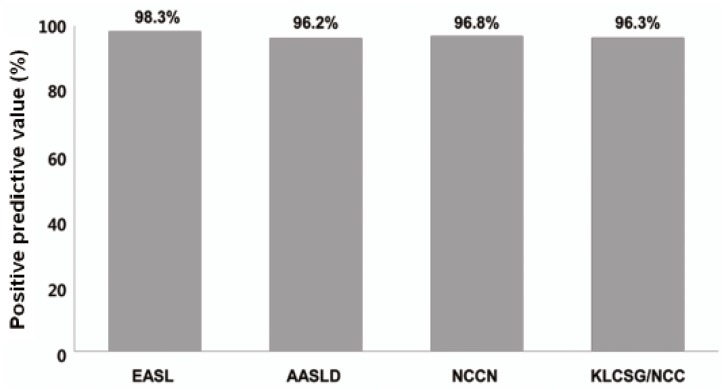
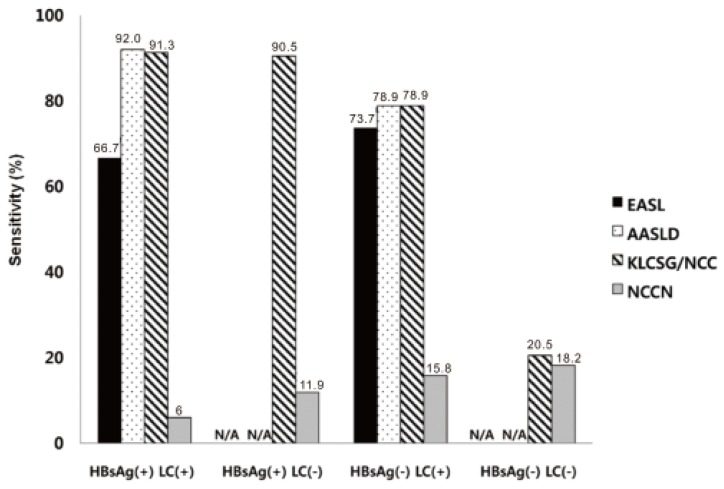
The overall sensitivity was highest using the KLCSG/NCC criteria (79.8%), followed by the AASLD (51.5%), EASL (38.4%), and NCCN (10.1%; P<0.001) criteria, whereas the specificity (84.5-98.3%) and positive predictive value (96.2-98.3%) were similar for all of the criteria. The KLCSG/NCC criteria had an acceptable false-positive rate and the highest sensitivity among all of the patients, including those positive for HBsAg, those without liver cancer, and those with a tumor of at least 2 cm.
The KLCSG/NCC and AASLD criteria exhibited the highest sensitivity, and all four guidelines had a high specificity among all of the patients. Based on the sensitivity and false-positive rate, the KLCSG/NCC criteria was the most useful in the majority of patients. Inclusion of HBV infection in the clinical diagnostic criteria for hepatocellular carcinoma would be reasonable and may lead to an improvement in the sensitivity, with acceptable false-positive rates, in HBV-endemic areas.
背景/目的:我们比较了乙型肝炎病毒(HBV)流行地区用于肝细胞癌的临床诊断标准的准确性和实用性。
我们回顾了 2008 年 1 月至 2009 年 12 月在我院接受肝切除术或肝活检的 355 例患者的病历。使用欧洲肝脏研究协会(EASL)、美国肝脏病研究协会(AASLD)、韩国肝癌研究组和国家癌症中心(KLCSG/NCC)和国家综合癌症网络(NCCN)指南提出的四种非侵入性肝细胞癌诊断标准对这些患者进行重新评估。
总体而言,KLCSG/NCC 标准的敏感性最高(79.8%),其次是 AASLD(51.5%)、EASL(38.4%)和 NCCN(10.1%;P<0.001),而特异性(84.5-98.3%)和阳性预测值(96.2-98.3%)在所有标准中相似。KLCSG/NCC 标准具有可接受的假阳性率和所有患者中最高的敏感性,包括 HBsAg 阳性患者、无肝癌患者和肿瘤至少 2cm 的患者。
KLCSG/NCC 和 AASLD 标准表现出最高的敏感性,所有四个指南在所有患者中均具有较高的特异性。基于敏感性和假阳性率,在大多数患者中,KLCSG/NCC 标准最为有用。将乙型肝炎病毒感染纳入肝细胞癌的临床诊断标准是合理的,可能会提高乙型肝炎病毒流行地区的敏感性,同时保持可接受的假阳性率。