Department of Paediatrics, University of Milano-Bicocca, Monza, Italy.
Lancet Oncol. 2012 Sep;13(9):936-45. doi: 10.1016/S1470-2045(12)70377-7. Epub 2012 Aug 14.
Trials of imatinib have provided evidence of activity in adults with Philadelphia-chromosome-positive acute lymphoblastic leukaemia (ALL), but the drug's role when given with multidrug chemotherapy to children is unknown. This study assesses the safety and efficacy of oral imatinib in association with a Berlin-Frankfurt-Munster intensive chemotherapy regimen and allogeneic stem-cell transplantation for paediatric patients with Philadelphia-chromosome-positive ALL.
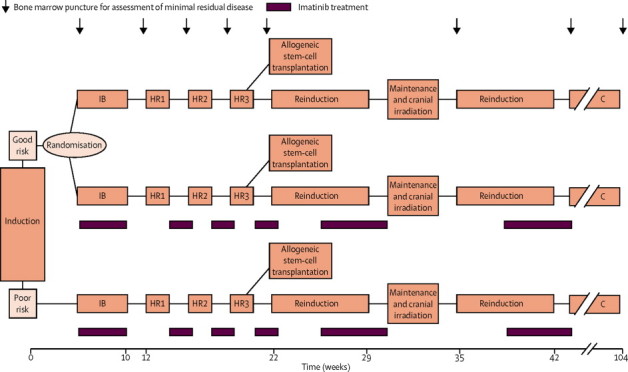
Patients aged 1-18 years recruited to national trials of front-line treatment for ALL were eligible if they had t(9;22)(q34;q11). Patients with abnormal renal or hepatic function, or an active systemic infection, were ineligible. Patients were enrolled by ten study groups between 2004 and 2009, and were classified as good risk or poor risk according to early response to induction treatment. Good-risk patients were randomly assigned by a web-based system with permuted blocks (size four) to receive post-induction imatinib with chemotherapy or chemotherapy only in a 1:1 ratio, while all poor-risk patients received post-induction imatinib with chemotherapy. Patients were stratified by study group. The chemotherapy regimen was modelled on a Berlin-Frankfurt-Munster high-risk backbone; all received four post-induction blocks of chemotherapy after which they became eligible for stem-cell transplantation. The primary endpoints were disease-free survival at 4 years in the good-risk group and event-free survival at 4 years in the poor-risk group, analysed by intention to treat and a secondary analysis of patients as treated. The trial is registered with EudraCT (2004-001647-30) and ClinicalTrials.gov, number NCT00287105.
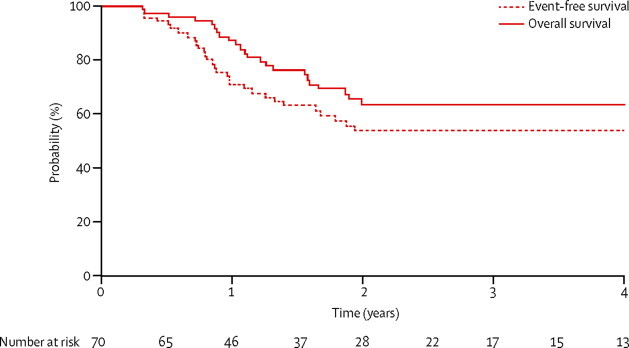
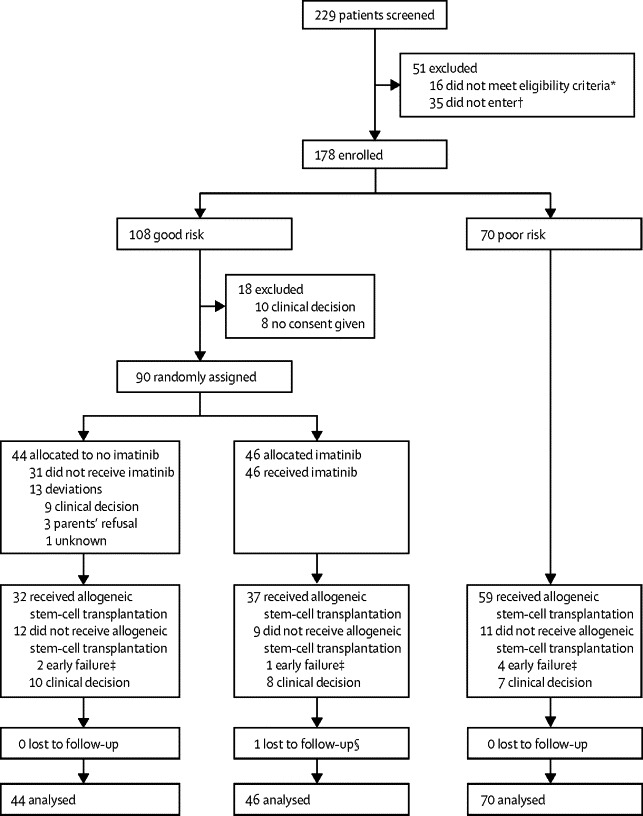
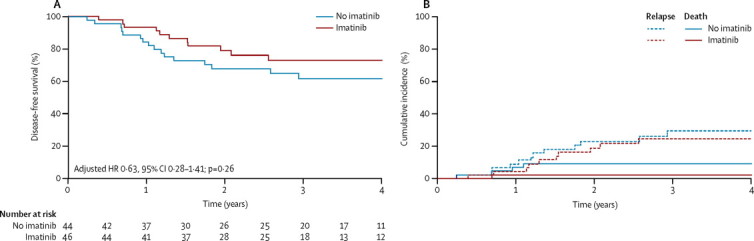
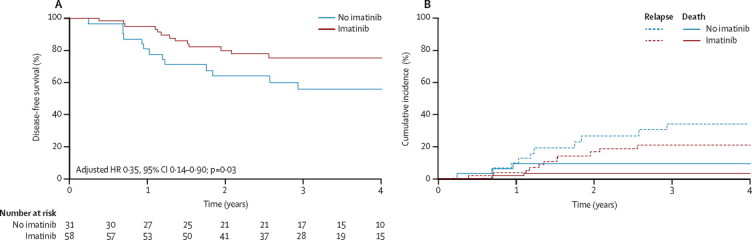
Between Jan 1, 2004, and Dec 31, 2009, we screened 229 patients and enrolled 178: 108 were good risk and 70 poor risk. 46 good-risk patients were assigned to receive imatinib and 44 to receive no imatinib. Median follow-up was 3·1 years (IQR 2·0-4·6). 4-year disease-free survival was 72·9% (95% CI 56·1-84·1) in the good-risk, imatinib group versus 61·7% (45·0-74·7) in the good-risk, no imatinib group (p=0·24). The hazard ratio (HR) for failure, adjusted for minimal residual disease, was 0·63 (0·28-1·41; p=0·26). The as-treated analysis showed 4-year disease-free survival was 75·2% (61·0-84·9) for good-risk patients receiving imatinib and 55·9% (36·1-71·7) for those who did not receive imatinib (p=0·06). 4-year event-free survival for poor-risk patients was 53·5% (40·4-65·0). Serious adverse events were much the same in the good-risk groups, with infections caused by myelosuppression the most common. 16 patients in the good-risk imatinib group versus ten in the good-risk, no imatinib group (p=0·64), and 24 in the poor-risk group, had a serious adverse event.
Our results suggests that imatinib in conjunction with intensive chemotherapy is well tolerated and might be beneficial for treatment of children with Philadelphia-chromosome-positive ALL.
Projet Hospitalier de Recherche Clinique-Cancer (France), Fondazione Tettamanti-De Marchi and Associazione Italiana per la Ricerca sul Cancro (Italy), Novartis Germany, Cancer Research UK, Leukaemia Lymphoma Research, and Central Manchester University Hospitals Foundation Trust.
伊马替尼的临床试验为费城染色体阳性急性淋巴细胞白血病(ALL)成人患者提供了疗效证据,但该药在儿童中与多药化疗联合应用的作用尚不清楚。本研究评估了口服伊马替尼联合柏林-法兰克福-慕尼黑强化化疗方案和同种异体造血干细胞移植在费城染色体阳性 ALL 儿科患者中的安全性和疗效。
参加 ALL 一线治疗国家试验的 1-18 岁患者,如果存在 t(9;22)(q34;q11),则符合入组条件。存在肾功能或肝功能异常或有全身活动性感染的患者不符合入组条件。本研究由十个研究组于 2004 年至 2009 年期间入组患者,并根据诱导治疗早期反应将患者分为低危和高危。采用基于互联网的随机区组(大小为 4)分配方案,低危患者随机分配接受诱导后伊马替尼联合化疗或单纯化疗,两组比例为 1:1,而所有高危患者均接受诱导后伊马替尼联合化疗。患者按研究组分层。化疗方案以柏林-法兰克福-慕尼黑高危方案为基础;所有患者在接受四个诱导后化疗周期后均有资格接受造血干细胞移植。主要终点是低危组的 4 年无病生存率和高危组的 4 年无事件生存率,分析方法为意向治疗和按治疗分析。该试验在 EudraCT(2004-001647-30)和 ClinicalTrials.gov 上注册,编号为 NCT00287105。
2004 年 1 月 1 日至 2009 年 12 月 31 日期间,我们筛选了 229 名患者,并入组了 178 名患者:108 名患者为低危,70 名患者为高危。46 名低危患者被分配接受伊马替尼治疗,44 名患者接受单纯化疗。中位随访时间为 3.1 年(IQR 2.0-4.6)。低危、伊马替尼组的 4 年无病生存率为 72.9%(95%CI 56.1-84.1),低危、无伊马替尼组为 61.7%(45.0-74.7)(p=0.24)。调整微小残留病后,失败的风险比(HR)为 0.63(0.28-1.41;p=0.26)。按治疗分析显示,接受伊马替尼治疗的低危患者 4 年无病生存率为 75.2%(61.0-84.9),未接受伊马替尼治疗的患者为 55.9%(36.1-71.7)(p=0.06)。高危患者的 4 年无事件生存率为 53.5%(40.4-65.0)。低危组的严重不良事件相似,最常见的是骨髓抑制引起的感染。低危伊马替尼组 16 例患者与低危、无伊马替尼组 10 例患者(p=0.64)和高危组 24 例患者发生严重不良事件。
我们的结果表明,伊马替尼联合强化化疗耐受性良好,可能对治疗费城染色体阳性 ALL 的儿童有益。
法国临床研究计划医院(Projet Hospitalier de Recherche Clinique-Cancer)、意大利 Tettamanti-De Marchi 和意大利癌症研究协会(Fondazione Tettamanti-De Marchi and Associazione Italiana per la Ricerca sul Cancro)、德国诺华公司(Novartis Germany)、英国癌症研究协会(Cancer Research UK)、英国白血病和淋巴瘤研究协会(Leukaemia Lymphoma Research)和英国中央曼彻斯特大学医院基金会信托基金(Central Manchester University Hospitals Foundation Trust)。