International Union Against Tuberculosis and Lung Disease, Paris, France.
J Int AIDS Soc. 2012;15(2):17396. doi: 17396.
Every year, HIV-associated tuberculosis (TB) deprives 350,000 mainly young people of productive and healthy lives.People die because TB is not diagnosed and treated in those with known HIV infection and HIV infection is not diagnosed in those with TB. Even in those in whom both HIV and TB are diagnosed and treated, this often happens far too late. These deficiencies can be addressed through the application of new scientific evidence and diagnostic tools.
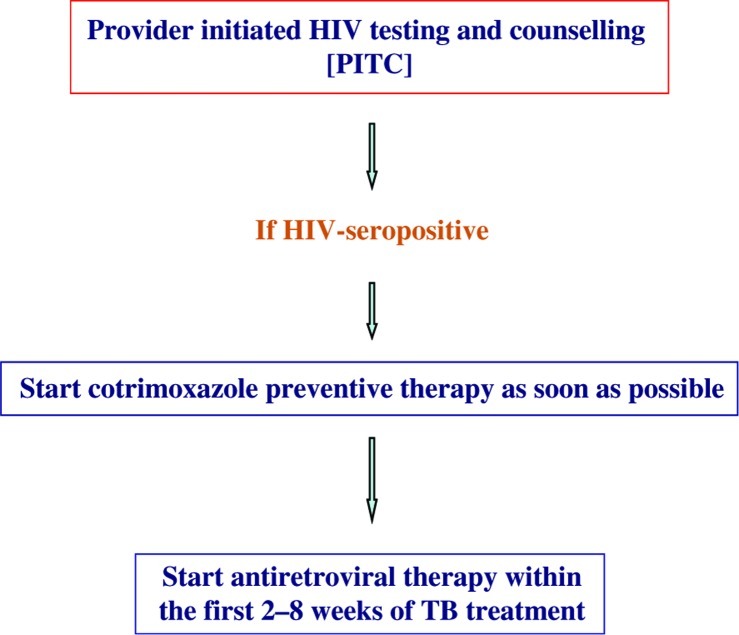
A strategy of starting antiretroviral therapy (ART) early in the course of HIV infection has the potential to considerably reduce both individual and community burden of TB and needs urgent evaluation for efficacy, feasibility and broader social and economic impact. Isoniazid preventive therapy can reduce the risk of TB and, if given strategically in addition to ART, provides synergistic benefit. Intensified TB screening as part of the "Three I's" strategy should be conducted at every clinic, home or community-based attendance using a symptoms-based algorithm, and new diagnostic tools should increasingly be used to confirm or refute TB diagnoses. Until such time when more sensitive and specific TB diagnostic assays are widely available, bolder approaches such as empirical anti-TB treatment need to be considered and evaluated. Patients with suspected or diagnosed TB must be screened for HIV and given cotrimoxazole preventive therapy and ART if HIV-positive. Three large randomized trials provide conclusive evidence that ART initiated within two to four weeks of start of anti-TB treatment saves lives, particularly in those with severe immunosuppression. The key to ensuring that these collaborative activities are delivered is the co-location and integration of TB and HIV services within the health system and the community.
Progress towards reducing HIV-associated TB deaths can be achieved through attention to simple and deliverable actions on the ground.
每年,艾滋病毒相关结核病(TB)使 35 万主要是年轻人丧失了富有成效和健康的生活。由于在已知 HIV 感染的人群中未诊断和治疗结核病,以及在有结核病的人群中未诊断 HIV 感染,人们因此而死亡。即使在那些同时诊断和治疗了 HIV 和 TB 的人群中,这种情况也常常发生得太晚。这些缺陷可以通过应用新的科学证据和诊断工具来解决。
在 HIV 感染过程中尽早开始抗逆转录病毒治疗(ART)的策略有可能大大减轻结核病的个人和社区负担,需要紧急评估其疗效、可行性以及更广泛的社会和经济影响。异烟肼预防性治疗可以降低结核病的风险,如果与 ART 一起进行策略性使用,可提供协同效益。强化结核病筛查应作为“三 I”策略的一部分,在每个诊所、家庭或社区就诊时进行,使用基于症状的算法,并应越来越多地使用新的诊断工具来确认或反驳结核病的诊断。在更敏感和更特异的结核病诊断检测广泛应用之前,需要考虑和评估更激进的方法,如经验性抗结核治疗。疑似或确诊结核病的患者必须接受 HIV 筛查,并在 HIV 阳性的情况下给予复方磺胺甲噁唑预防治疗和 ART。三项大型随机试验提供了确凿的证据,表明在开始抗结核治疗的 2 至 4 周内启动 ART 可挽救生命,特别是在严重免疫抑制的患者中。确保这些协作活动得以实施的关键是在卫生系统和社区内将结核病和 HIV 服务置于同一地点并进行整合。
通过关注地面上简单易行的行动,可以实现减少与艾滋病毒相关的结核病死亡的目标。