Division of Nephrology, Department of Medicine, Taipei Veterans General Hospital, Taipei, Taiwan.
BMC Nephrol. 2012 Aug 23;13:89. doi: 10.1186/1471-2369-13-89.
The renin-angiotensin-aldosterone system (RAAS) plays an important role in the progression of chronic kidney disease (CKD). Although dual RAAS inhibition results in worse renal outcomes than monotherapy in high risk type 2 diabetes patients, the effect of dual RAAS inhibition in patients with non-DM CKD is unclear. The aim of this study was to evaluate the potential renoprotective effect of add-on direct renin inhibitor in non-DM CKD patients.
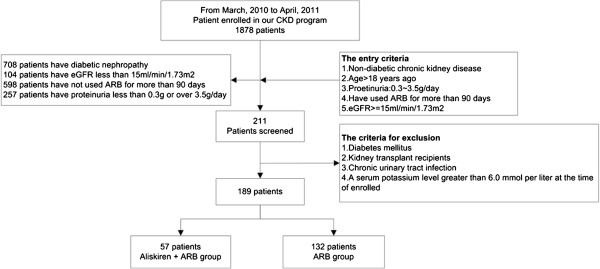
We retrospectively enrolled 189 non-DM CKD patients who had been taking angiotensin II receptor blockers (ARBs) for more than six months. Patients were divided into an add-on aliskiren group and an ARB monotherapy group. The primary outcomes were a decline in glomerular filtration rate (GFR) and a reduction in urinary protein-to-creatinine ratio at six months.
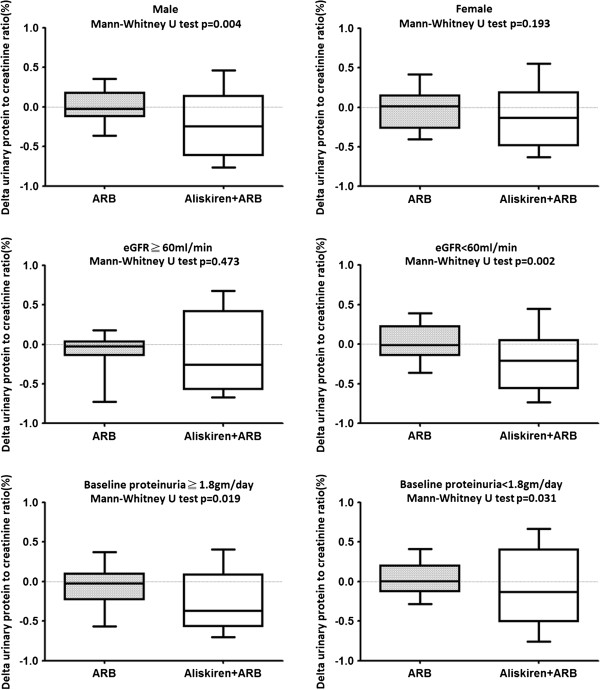
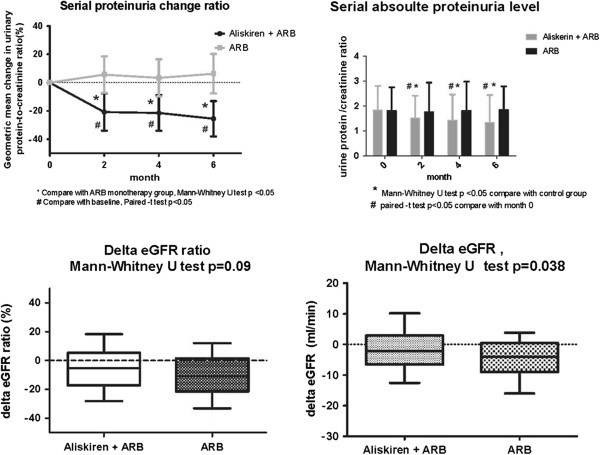
The baseline characteristics of the two groups were similar. Aliskiren 150 mg daily reduced the urinary protein-to-creatinine ratio by 26% (95% confidence interval, 15 to 37%; p < 0.001). The decline in GFR was smaller in the add-on aliskiren group (-2.1 vs. -4.0 ml/min, p = 0.038). Add-on aliskiren had a neutral effect on serum potassium in the non-DM CKD patients. In subgroup analysis, the proteinuria-reducing effect of aliskiren was more prominent in patients with a GFR less than 60 ml/min, and in patients with a urinary protein-to-creatinine ratio greater than 1.8. The effect of aliskiren in retarding the decline in GFR was more prominent in patients with hypertensive nephropathy than in those with glomerulonephritis.
Add-on direct renin inhibitor aliskiren (150 mg daily) safely reduced proteinuria and attenuated the decline in GFR in the non-DM CKD patients who were receiving ARBs.
肾素-血管紧张素-醛固酮系统(RAAS)在慢性肾脏病(CKD)的进展中起着重要作用。尽管双重 RAAS 抑制在高危 2 型糖尿病患者中的肾脏结局比单药治疗更差,但双重 RAAS 抑制在非糖尿病 CKD 患者中的效果尚不清楚。本研究旨在评估非糖尿病 CKD 患者中添加直接肾素抑制剂的潜在肾脏保护作用。
我们回顾性纳入了 189 名已服用血管紧张素 II 受体阻滞剂(ARBs)超过 6 个月的非糖尿病 CKD 患者。患者分为添加阿利克仑组和 ARB 单药治疗组。主要结局是 6 个月时肾小球滤过率(GFR)下降和尿蛋白与肌酐比值降低。
两组的基线特征相似。阿利克仑 150mg 每日可使尿蛋白与肌酐比值降低 26%(95%置信区间,15 至 37%;p < 0.001)。添加阿利克仑组 GFR 下降幅度较小(-2.1 与-4.0ml/min,p = 0.038)。添加阿利克仑对非糖尿病 CKD 患者的血清钾无影响。亚组分析显示,阿利克仑在 GFR 低于 60ml/min 的患者和尿蛋白与肌酐比值大于 1.8 的患者中具有更显著的蛋白尿减少作用。阿利克仑对 GFR 下降的减缓作用在高血压性肾病患者中比在肾小球肾炎患者中更为显著。
添加直接肾素抑制剂阿利克仑(每日 150mg)可安全降低非糖尿病 CKD 患者接受 ARB 治疗时的蛋白尿,并减缓 GFR 下降。