Section of Chronic Disease Epidemiology, Department of Epidemiology and Public Health, Yale University School of Medicine, New Haven, CT 06520-8034, USA.
Stroke. 2012 Oct;43(10):2741-7. doi: 10.1161/STROKEAHA.112.665646. Epub 2012 Aug 30.
The critical access hospital (CAH) designation was established to provide rural residents with local access to emergency and inpatient care. CAHs, however, have poorer short-term outcomes for pneumonia, heart failure, and myocardial infarction compared with other hospitals. We assessed whether 30-day risk-standardized mortality rates (RSMRs) and risk-standardized readmission rates (RSRRs) after ischemic stroke differ between CAHs and non-CAHs.
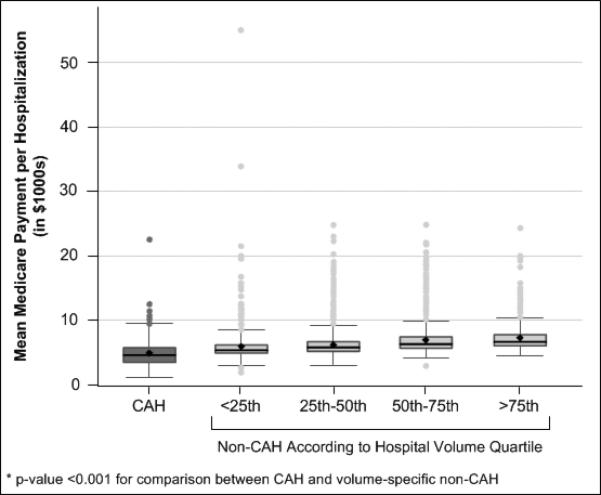
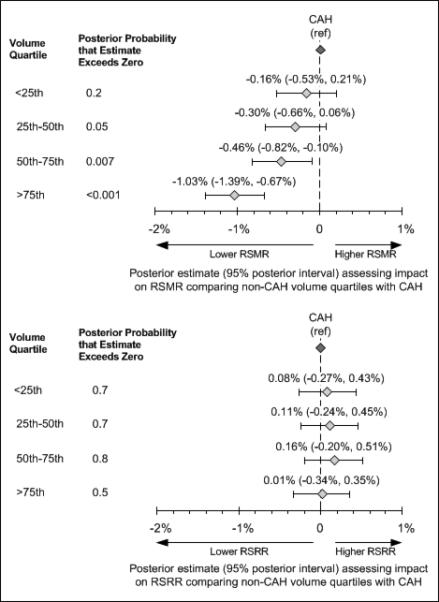
The study included all fee-for-service Medicare beneficiaries 65 years of age or older with a primary discharge diagnosis of ischemic stroke (International Classification of Diseases, 9th revision codes 433, 434, 436) in 2006. Hierarchical generalized linear models calculated hospital-level RSMRs and RSRRs, adjusting for patient demographics, medical history, and comorbid conditions. Non-CAHs were categorized by hospital volume quartiles and the RSMR and RSRR posterior probabilities in comparison with CAHs were determined using linear regression with Markov chain Monte Carlo simulation.
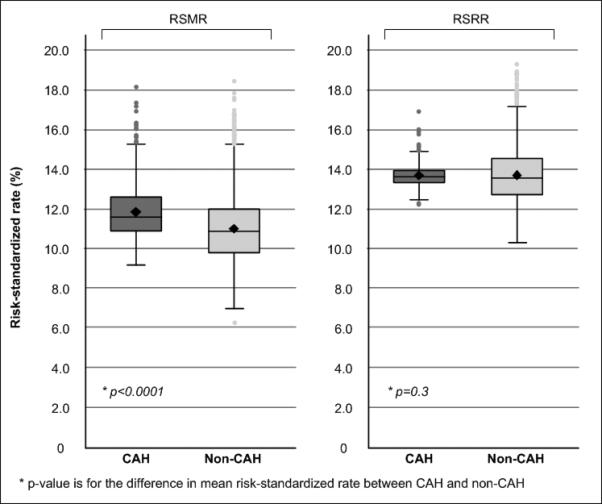
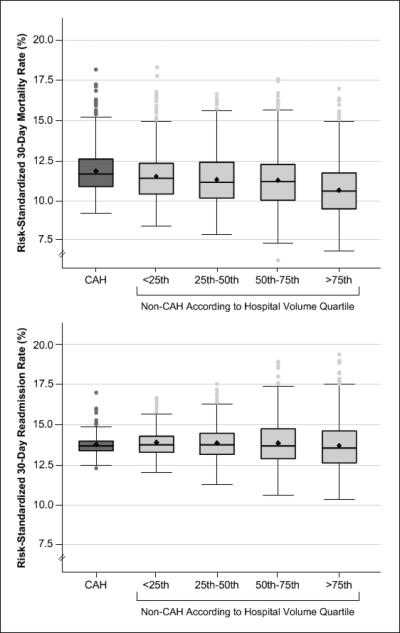
There were 10 267 ischemic stroke discharges from 1165 CAHs and 300 114 discharges from 3381 non-CAHs. The RSMRs of CAHs were higher than non-CAHs (11.9%± 1.4% vs 10.9%± 1.7%; P<0.001), but the RSRRs were comparable (13.7%± 0.6% vs 13.7%± 1.4%; P=0.3). The RSMRs for the 2 higher volume quartiles of non-CAHs were lower than CAHs (posterior probability of RSMRs higher than CAHs=0.007 for quartile 3; P<0.001 for quartile 4), but there were no differences for lower volume hospitals; RSRRs did not vary by annual hospital volume.
CAHs had higher RSMRs compared with non-CAHs, but readmission rates were similar. The observed differences may be partly explained by patient characteristics and annual hospital volume.
建立基层医疗机构(CAH)的目的是为农村居民提供当地获得急诊和住院治疗的机会。然而,与其他医院相比,CAH 治疗肺炎、心力衰竭和心肌梗死的短期预后更差。我们评估了缺血性卒中后 30 天风险标准化死亡率(RSMR)和风险标准化再入院率(RSRR)是否在 CAH 和非 CAH 之间存在差异。
本研究纳入了所有在 2006 年因主要诊断为缺血性卒中(国际疾病分类第 9 版代码 433、434、436)而接受按服务收费的 Medicare 受益人的数据。使用分层广义线性模型计算医院水平的 RSMR 和 RSRR,并调整了患者的人口统计学、病史和合并症。非 CAH 按医院容量四分位数进行分类,并通过带有马尔可夫链蒙特卡罗模拟的线性回归确定与 CAH 相比的 RSMR 和 RSRR 后验概率。
共有 1165 家 CAH 和 3381 家非 CAH 的 10267 例缺血性卒中出院患者和 300114 例出院患者。CAH 的 RSMR 高于非 CAH(11.9%±1.4%比 10.9%±1.7%;P<0.001),但 RSRR 相当(13.7%±0.6%比 13.7%±1.4%;P=0.3)。非 CAH 中前 2 个高容量四分位数的 RSMR 低于 CAH(第 3 四分位数的 RSMR 高于 CAH 的后验概率为 0.007;第 4 四分位数为 P<0.001),而低容量医院则无差异;医院年容量对 RSRR 没有影响。
CAH 的 RSMR 高于非 CAH,但再入院率相似。观察到的差异可能部分归因于患者特征和医院年容量。