Center for Evidence-based Practice, University of Pennsylvania, Suite 50 Mezzanine, 3535 Market Street, Philadelphia, PA, USA.
BMC Med Inform Decis Mak. 2012 Aug 31;12:92. doi: 10.1186/1472-6947-12-92.
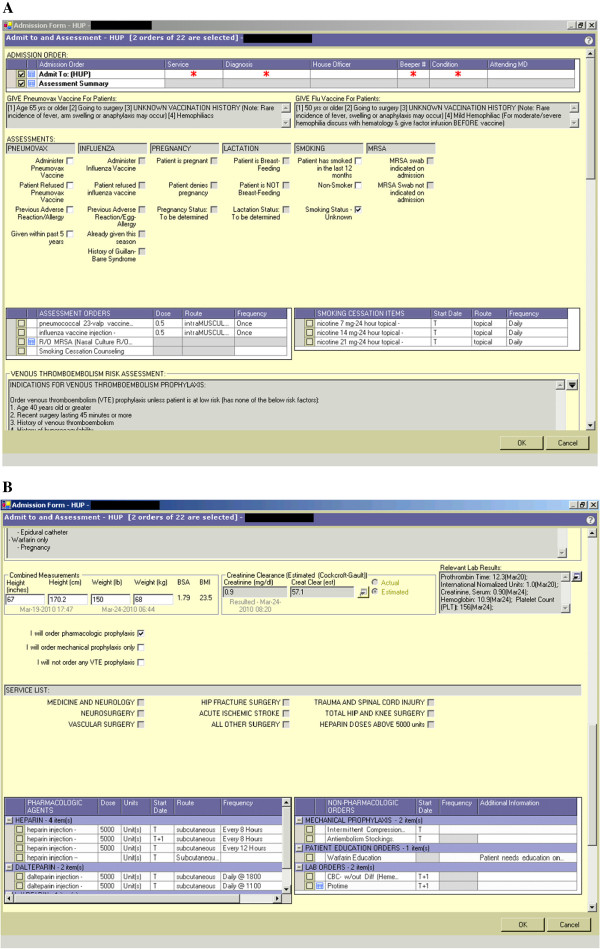
Venous thromboembolism (VTE) causes morbidity and mortality in hospitalized patients, and regulators and payors are encouraging the use of systems to prevent them. Here, we examine the effect of a computerized clinical decision support (CDS) intervention implemented across a multi-hospital academic health system on VTE prophylaxis and events.
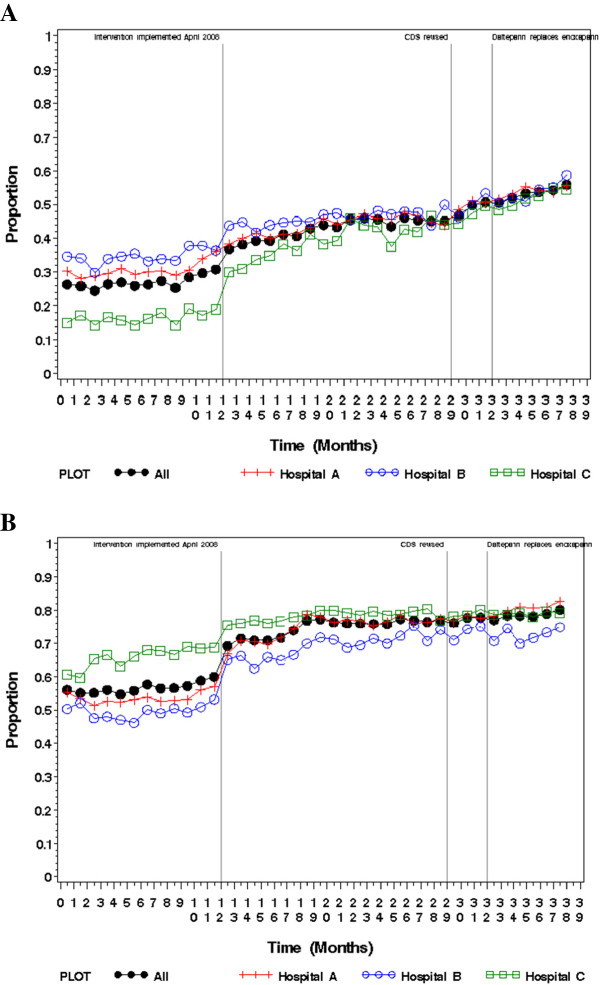
The study included 223,062 inpatients admitted between April 2007 and May 2010, and used administrative and clinical data. The intervention was integrated into a commercial electronic health record (EHR) in an admission orderset used for all admissions. Three time periods were examined: baseline (period 1), and the time after implementation of the first CDS intervention (period 2) and a second iteration (period 3). Providers were prompted to accept or decline prophylaxis based on patient risk. Time series analyses examined the impact of the intervention on VTE prophylaxis during time periods two and three compared to baseline, and a simple pre-post design examined impact on VTE events and bleeds secondary to anticoagulation. VTE prophylaxis and events were also examined in a prespecified surgical subset of our population meeting the public reporting criteria defined by the Agency for Healthcare Research and Quality (AHRQ) Patient Safety Indicator (PSI).
Unadjusted analyses suggested that "recommended", "any", and "pharmacologic" prophylaxis increased from baseline to the last study period (27.1% to 51.9%, 56.7% to 78.1%, and 42.0% to 54.4% respectively; p < 0.01 for all comparisons). Results were significant across all hospitals and the health system overall. Interrupted time series analyses suggested that our intervention increased the use of "recommended" and "any" prophylaxis by 7.9% and 9.6% respectively from baseline to time period 2 (p < 0.01 for both comparisons); and 6.6% and 9.6% respectively from baseline to the combined time periods 2 and 3 (p < 0.01 for both comparisons). There were no significant changes in "pharmacologic" prophylaxis in the adjusted model. The overall percent of patients with VTE increased from baseline to the last study period (2.0% to 2.2%; p = 0.03), but an analysis excluding patients with VTE "present on admission" (POA) demonstrated no difference in events (1.3% to 1.3%; p = 0.80). Overall bleeds did not significantly change. An analysis examining VTE prophylaxis and events in a surgical subset of patients defined by the AHRQ PSI demonstrated increased "recommended", "any", and "pharmacologic" prophylaxis from baseline to the last study period (32.3% to 60.0%, 62.8% to 85.7%, and 47.9% to 63.3% respectively; p < 0.01 for all comparisons) as well as reduced VTE events (2.2% to 1.7%; p < 0.01).
The CDS intervention was associated with an increase in "recommended" and "any" VTE prophylaxis across the multi-hospital academic health system. The intervention was also associated with increased VTE rates in the overall study population, but a subanalysis using only admissions with appropriate POA documentation suggested no change in VTE rates, and a prespecified analysis of a surgical subset of our sample as defined by the AHRQ PSI for public reporting purposes suggested reduced VTE. This intervention was created in a commonly used commercial EHR and is scalable across institutions with similar systems.
静脉血栓栓塞症(VTE)可导致住院患者发病和死亡,监管机构和支付方鼓励使用系统来预防 VTE。在这里,我们研究了在多医院学术医疗系统中实施的计算机临床决策支持(CDS)干预对 VTE 预防和事件的影响。
该研究纳入了 2007 年 4 月至 2010 年 5 月期间入院的 223062 名住院患者,使用了行政和临床数据。干预措施整合到了一个商业电子健康记录(EHR)中,该 EHR 用于所有入院患者的入院医嘱集。研究考察了三个时期:基线期(第 1 期)、首次 CDS 干预实施后的时期(第 2 期)和第二次迭代时期(第 3 期)。根据患者风险,医生会被提示接受或拒绝预防措施。时间序列分析考察了干预对第 2 期和第 3 期与基线期相比的 VTE 预防的影响,简单的前后设计考察了抗凝治疗继发性 VTE 事件和出血的影响。还在我们的人群中符合美国医疗保健研究与质量局(AHRQ)患者安全指标(PSI)定义的公共报告标准的一个特定手术亚组中检查了 VTE 预防和事件。
未调整分析表明,“推荐”、“任何”和“药物”预防从基线期增加到最后研究期(分别从 27.1%增加到 51.9%、56.7%增加到 78.1%和 42.0%增加到 54.4%;所有比较均 P<0.01)。结果在所有医院和整个医疗系统中均具有统计学意义。中断时间序列分析表明,我们的干预措施使“推荐”和“任何”预防的使用分别增加了 7.9%和 9.6%,从基线期到第 2 期(所有比较均 P<0.01);从基线期到第 2 期和第 3 期的综合时期分别增加了 6.6%和 9.6%(所有比较均 P<0.01)。调整模型中药物预防没有显著变化。总的 VTE 患者百分比从基线期增加到最后研究期(从 2.0%增加到 2.2%;P=0.03),但排除 VTE“入院时即存在”(POA)的患者的分析显示事件没有差异(从 1.3%增加到 1.3%;P=0.80)。总的出血没有显著变化。对符合 AHRQ PSI 的手术亚组患者的 VTE 预防和事件的分析表明,“推荐”、“任何”和“药物”预防从基线期增加到最后研究期(从 32.3%增加到 60.0%、从 62.8%增加到 85.7%和从 47.9%增加到 63.3%;所有比较均 P<0.01),同时减少了 VTE 事件(从 2.2%减少到 1.7%;P<0.01)。
CDS 干预措施与多医院学术医疗系统中“推荐”和“任何”VTE 预防的增加有关。该干预措施还与总体研究人群的 VTE 发生率增加有关,但使用仅具有适当 POA 记录的入院患者的亚分析表明 VTE 发生率没有变化,对我们样本中符合 AHRQ PSI 用于公共报告目的的手术亚组的预设分析表明 VTE 减少。该干预措施是在常用的商业 EHR 中创建的,可在具有类似系统的机构中扩展。