David Geffen School of Medicine, University of California Los Angeles, Los Angeles, California, United States of America.
PLoS One. 2012;7(9):e41212. doi: 10.1371/journal.pone.0041212. Epub 2012 Sep 5.
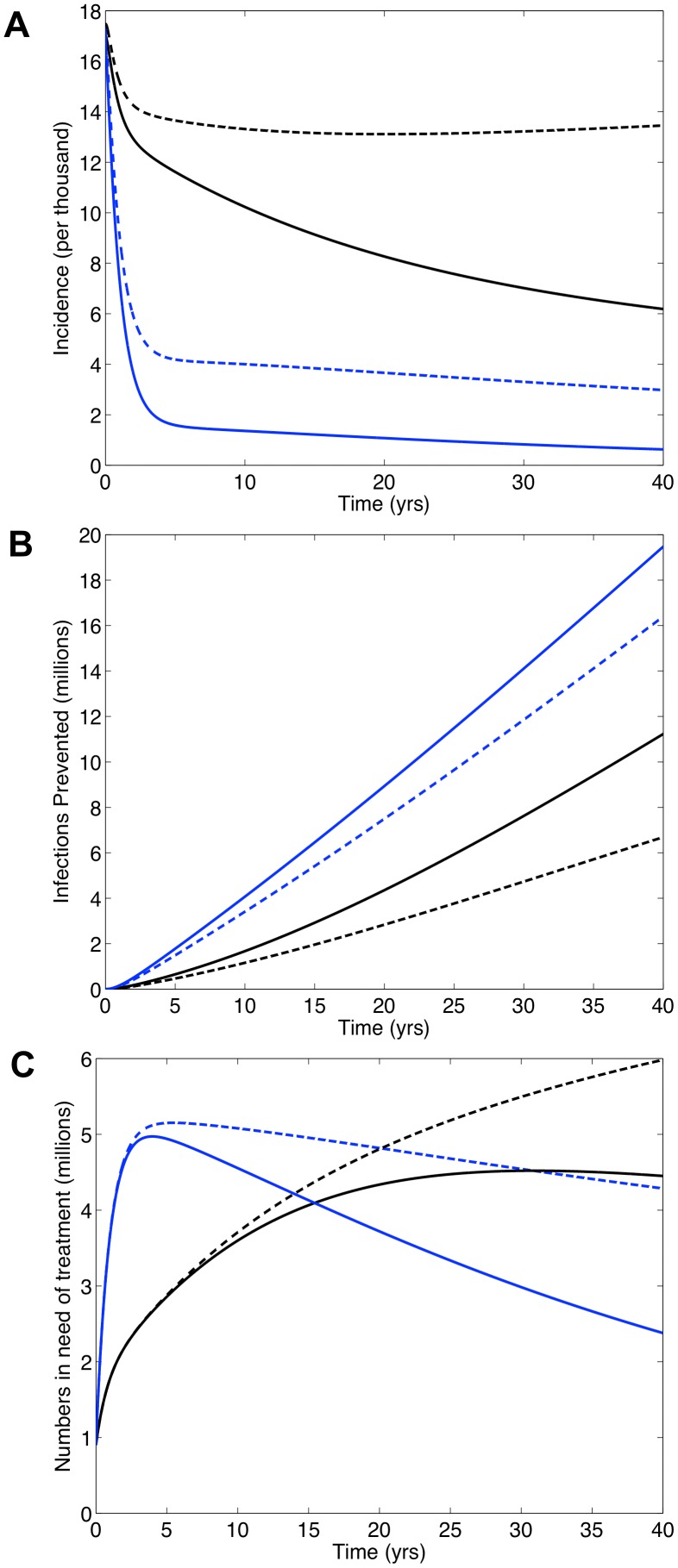
In South Africa (SA) universal access to treatment for HIV-infected individuals in need has yet to be achieved. Currently ~1 million receive treatment, but an additional 1.6 million are in need. It is being debated whether to use a universal 'test and treat' (T&T) strategy to try to eliminate HIV in SA; treatment reduces infectivity and hence transmission. Under a T&T strategy all HIV-infected individuals would receive treatment whether in need or not. This would require treating 5 million individuals almost immediately and providing treatment for several decades. We use a validated mathematical model to predict impact and costs of: (i) a universal T&T strategy and (ii) achieving universal access to treatment. Using modeling the WHO has predicted a universal T&T strategy in SA would eliminate HIV within a decade, and (after 40 years) cost ~$10 billion less than achieving universal access. In contrast, we predict a universal T&T strategy in SA could eliminate HIV, but take 40 years and cost ~$12 billion more than achieving universal access. We determine the difference in predictions is because the WHO has under-estimated survival time on treatment and ignored the risk of resistance. We predict, after 20 years, ~2 million individuals would need second-line regimens if a universal T&T strategy is implemented versus ~1.5 million if universal access is achieved. Costs need to be realistically estimated and multiple evaluation criteria used to compare 'treatment as prevention' with other prevention strategies. Before implementing a universal T&T strategy, which may not be sustainable, we recommend striving to achieve universal access to treatment as quickly as possible. We predict achieving universal access to treatment would be a very effective 'treatment as prevention' approach and bring the HIV epidemic in SA close to elimination, preventing ~4 million infections after 20 years and ~11 million after 40 years.
在南非(SA),尚未实现为所有需要的 HIV 感染者提供治疗的普遍获取。目前约有 100 万人接受治疗,但仍有 160 万人需要治疗。目前正在争论是否采用普遍的“检测和治疗”(T&T)策略来尝试在南非消除 HIV;治疗可降低传染性,从而减少传播。根据 T&T 策略,所有 HIV 感染者无论是否需要,都将接受治疗。这将需要立即治疗 500 万人,并在未来几十年内提供治疗。我们使用经过验证的数学模型来预测以下两种策略的影响和成本:(i)普遍 T&T 策略,以及(ii)实现普遍治疗。世界卫生组织(WHO)通过建模预测,在南非实施普遍 T&T 策略将在十年内消除 HIV,且(40 年后)比实现普遍治疗节省约 100 亿美元。相比之下,我们预测在南非实施普遍 T&T 策略可能会消除 HIV,但需要 40 年时间,且比实现普遍治疗多花费约 120 亿美元。我们确定预测结果的差异在于,世界卫生组织低估了治疗中的生存时间,并忽略了耐药的风险。我们预测,如果实施普遍 T&T 策略,20 年后约有 200 万人需要二线方案,而如果实现普遍治疗,约有 150 万人需要二线方案。需要对成本进行现实的评估,并使用多个评估标准来比较“治疗即预防”与其他预防策略。在实施可能不可持续的普遍 T&T 策略之前,我们建议尽快努力实现普遍治疗。我们预测实现普遍治疗将是一种非常有效的“治疗即预防”方法,可使南非的 HIV 疫情接近消除,在 20 年后预防约 400 万人感染,在 40 年后预防约 1100 万人感染。