Department of Medicine and Public Health, Alma Mater Studiorum, University of Bologna, Bologna, 40126, Italy.
BMC Health Serv Res. 2012 Sep 10;12:310. doi: 10.1186/1472-6963-12-310.
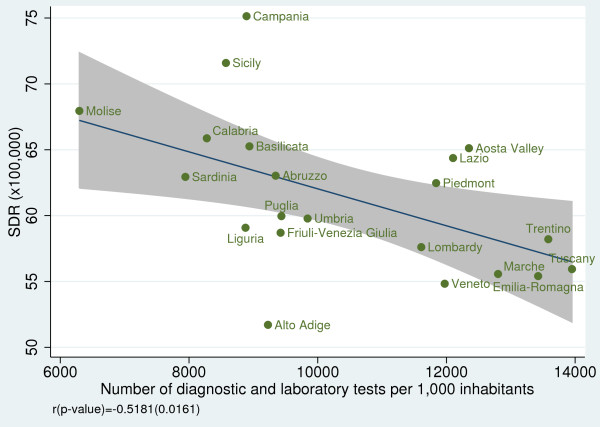
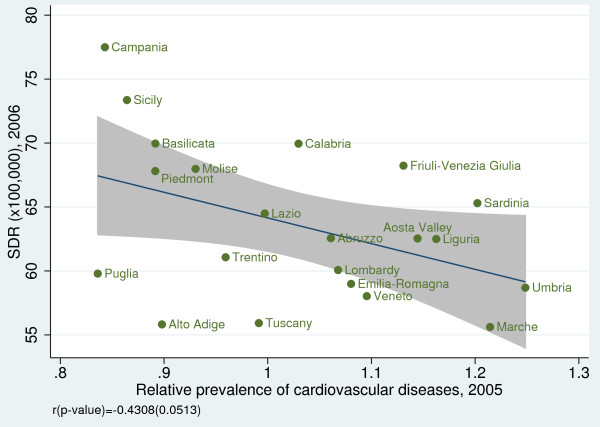
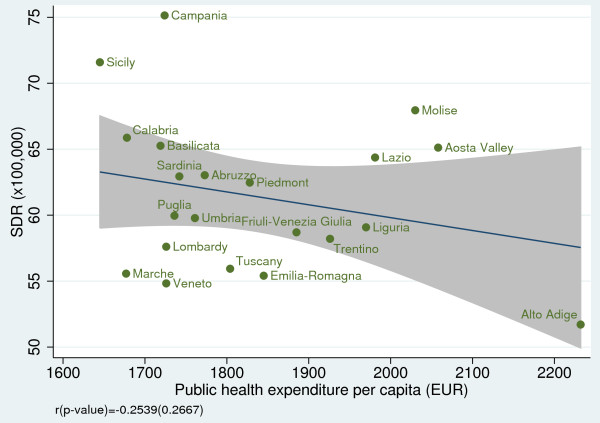
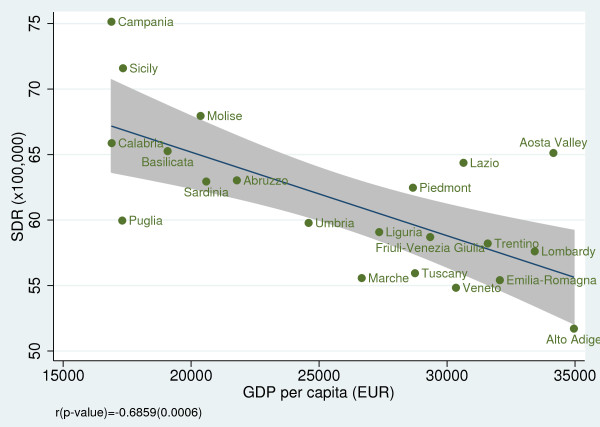
Mortality amenable to health-care services ('amenable mortality') has been defined as "premature deaths that should not occur in the presence of timely and effective health care" and as "conditions for which effective clinical interventions exist." We analyzed the regional variability in health-care services using amenable mortality as a performance indicator. Convergent validity was examined against other indicators, such as health expenditure, GDP per capita, life expectancy at birth, disability-free life expectancy at age 15, number of diagnostic and laboratory tests per 1,000 inhabitants, and the prevalence of cancer and cardiovascular diseases.
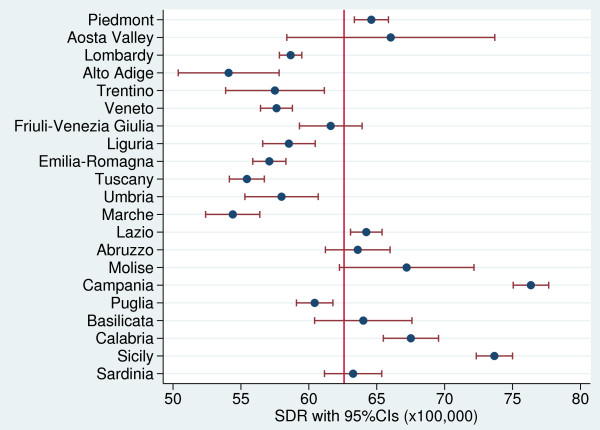
Amenable mortality rate was calculated as the average annual number of deaths in the population aged 0-74 years per 100,000 inhabitants, and it was then stratified by gender and region. Data were drawn from national mortality statistics for the period 2006-08.
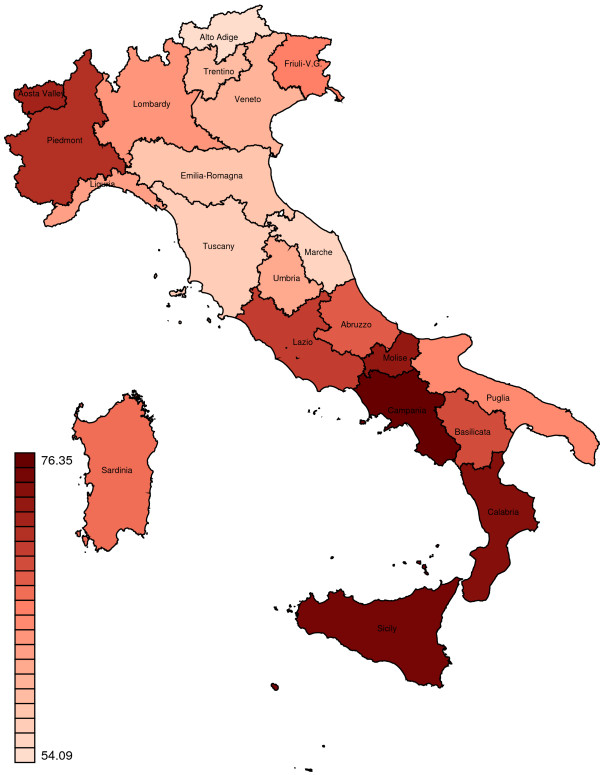
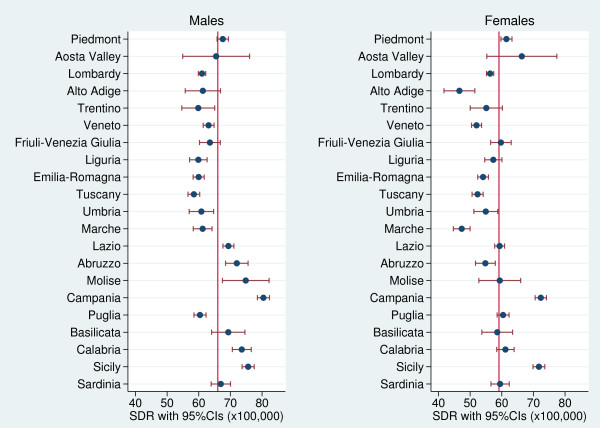
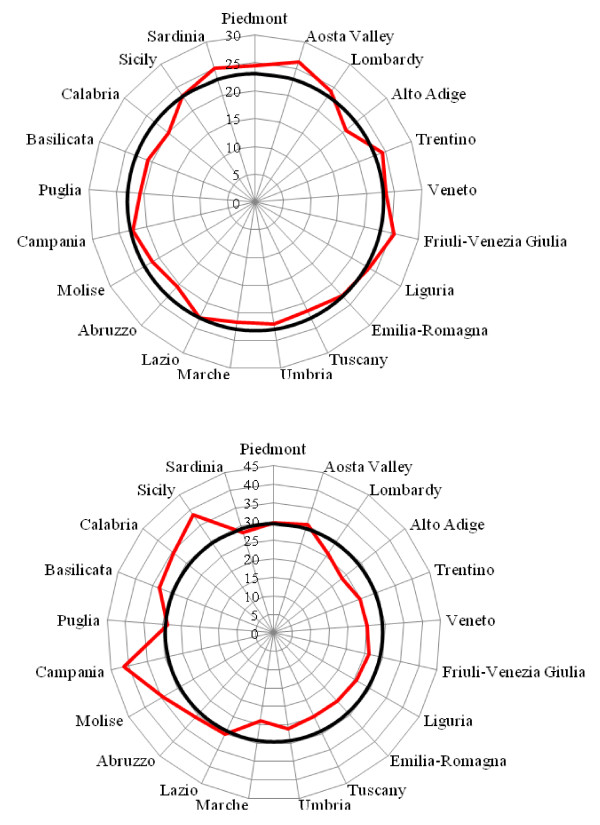
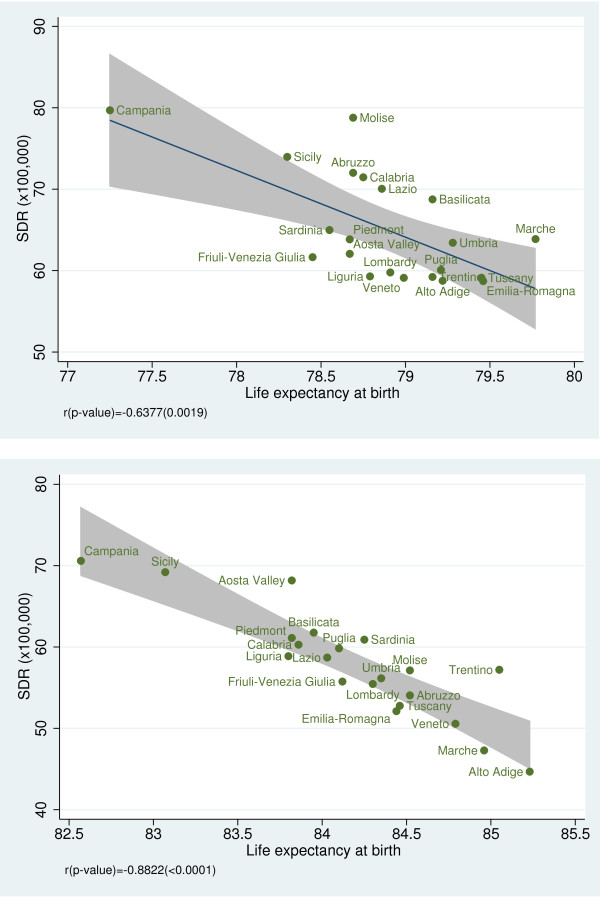
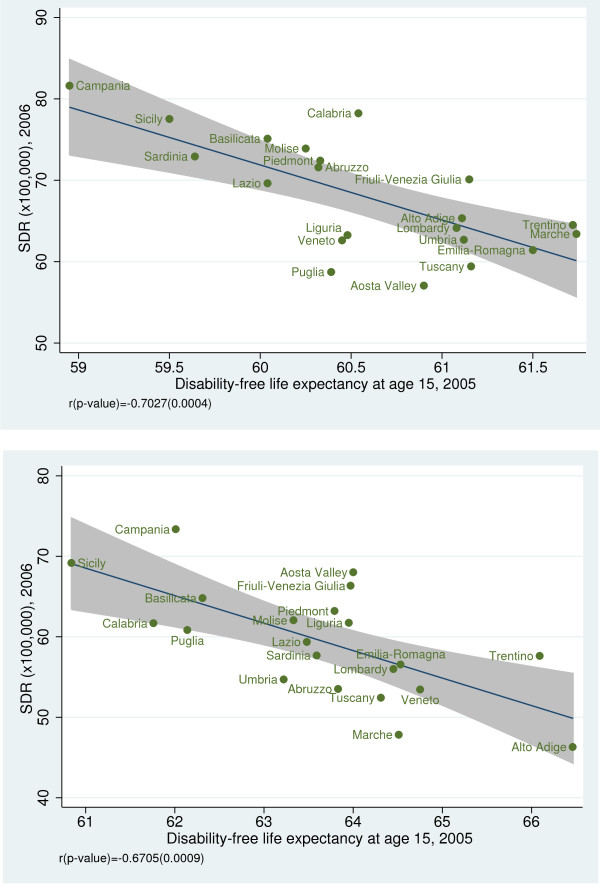
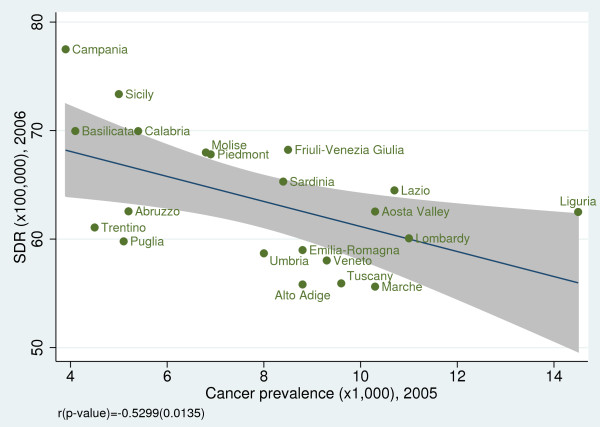
During the study period (2006-08), the age-standardized death rate (SDR) amenable to health-care services in Italy was 62.6 per 100,000 inhabitants: 66.0 per 100,000 for males and 59.1 per 100,000 for females. Significant regional variations ranged from 54.1 per 100,000 inhabitants in Alto Adige to 76.3 per 100,000 in Campania. Regional variability in SDR was examined separately for male and females. The variability proved to be statistically significant for both males and females (males: Q-test = 638.5, p < 0.001; females: Q-test = 700.1, p < 0.001). However, among men, we found a clear-cut divide in SDR values between Central and Southern Italy; among women, this divide was less pronounced. Amenable mortality was negatively correlated with life expectancy at birth for both genders (male: r = -0.64, p = 0.002; female: r = -0.88, p <0.001) and with disability-free life expectancy at age 15 (male: r = -0.70, p <0.001; female: r = -0.67, p <0.001). Amenable mortality displayed a statistically significant negative relationship with GDP per capita, the quantity of diagnostic and laboratory tests per 1,000 inhabitants, and the prevalence of cancer.
Amenable mortality shows a wide variation across Italian regions and an inverse relationship with life expectancy and GDP per capita, as expected.
可归因于医疗保健服务的死亡率(“可归因死亡率”)被定义为“在及时和有效的医疗保健存在的情况下,不应该发生的过早死亡”和“存在有效临床干预的情况”。我们使用可归因死亡率作为绩效指标来分析区域间医疗保健服务的差异。收敛有效性是通过其他指标来检验的,如卫生支出、人均国内生产总值、出生时的预期寿命、15 岁时无残疾预期寿命、每 1000 居民的诊断和实验室检查数量以及癌症和心血管疾病的患病率。
可归因死亡率率计算为每 100000 名 0-74 岁人群中每年的平均死亡人数,然后按性别和地区进行分层。数据来自 2006-08 年的国家死亡率统计数据。
在研究期间(2006-08 年),意大利的医疗保健服务可归因的标准化死亡率(SDR)为每 100000 居民 62.6 人:男性为每 100000 居民 66.0 人,女性为每 100000 居民 59.1 人。从 54.1 人/100000 居民在阿迪杰到 76.3 人/100000 居民在坎帕尼亚,地区差异显著。分别为男性和女性检查 SDR 的地区差异。对于男性和女性,这种差异具有统计学意义(男性:Q 检验=638.5,p<0.001;女性:Q 检验=700.1,p<0.001)。然而,在男性中,我们发现中南部意大利的 SDR 值之间存在明显的差异;在女性中,这种差异不那么明显。可归因死亡率与出生时的预期寿命呈负相关,对于两性(男性:r=-0.64,p=0.002;女性:r=-0.88,p<0.001)和 15 岁时的无残疾预期寿命(男性:r=-0.70,p<0.001;女性:r=-0.67,p<0.001)。可归因死亡率与人均国内生产总值、每 1000 居民的诊断和实验室检查数量以及癌症的患病率呈统计学显著负相关。
可归因死亡率在意大利各地区差异很大,与预期的预期寿命和人均国内生产总值呈负相关。