Wnent Jan, Seewald Stephan, Heringlake Matthias, Lemke Hans, Brauer Kirk, Lefering Rolf, Fischer Matthias, Jantzen Tanja, Bein Berthold, Messelken Martin, Gräsner Jan-Thorsten
Crit Care. 2012 Sep 12;16(5):R164. doi: 10.1186/cc11516.
Between 1 and 31% of patients suffering out-of-hospital cardiac arrest (OHCA) survive to discharge from hospital. International studies have shown that the level of care provided by the admitting hospital determines survival for patients suffering from OHCA. These data may only be partially transferable to the German medical system where responders are in-field emergency medical physicians. The present study determines the influence of the emergency physician's choice of admitting hospital on patient outcome after OHCA in a large urban setting.
All data for patients collected in the German Resuscitation Registry for the city of Dortmund during 2007 and 2008 were analyzed. Patients under 18 years of age, with traumatic mechanism, and with incomplete charts were excluded. Admitting hospitals were divided into two groups: those without the capability for percutaneous coronary intervention (PCI), and those with PCI capability. Data were analyzed by multivariate statistics, taking into account the effects of mild therapeutic hypothermia treatment and PCI capability of the admitting hospital with respect to the neurological status upon hospital discharge.
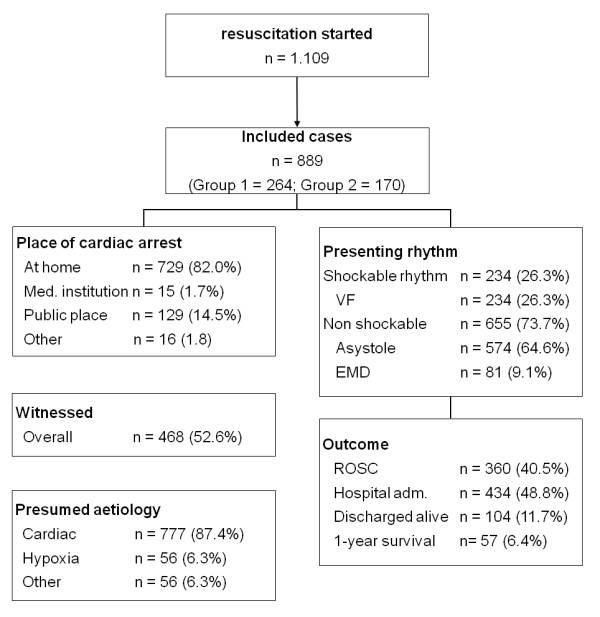
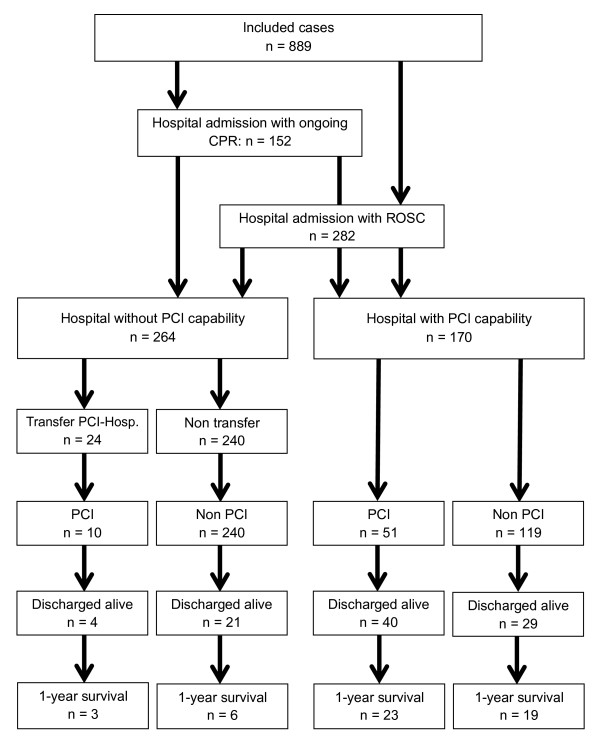
Between 2007 and 2008 a total of 1,109 cardiopulmonary resuscitation attempts were registered for the city of Dortmund, of which 889 could be included in our study. Return of spontaneous circulation was achieved in 360 of 889 patients (40.5%). In total, 282 of 889 patients displayed return of spontaneous circulation during transport to the hospital (31.7%); 152 were transported with ongoing cardiopulmonary resuscitation (17.1%). Of the total 434 patients admitted to hospital, 264 were admitted to hospitals without PCI capability and 170 to hospitals with PCI capability. Multivariate analysis demonstrated a significant influence on patient discharge with good neurological status for those admitted to PCI hospitals (odds ratio 3.14 (95% confidence interval 1.51 to 6.56)), independent of receiving mild therapeutic hypothermia and/or PCI. Compared with patients admitted to hospitals without PCI capability, significantly more patients in PCI hospitals were discharged alive (41% vs. 13%, P < 0.001) and remained alive 1 year after the event (28% vs. 6%, P < 0.001).
The choice of admitting hospital for patients suffering OHCA significantly influences treatment and outcome. This influence is independent of PCI performance and of mild therapeutic hypothermia. Further analysis is required to determine the possible parameters determining patient outcome.
院外心脏骤停(OHCA)患者中,1%至31%可存活至出院。国际研究表明,收治医院提供的护理水平决定了OHCA患者的存活情况。这些数据可能仅部分适用于德国医疗系统,在德国,现场急救人员为急诊内科医生。本研究确定了在大城市环境中,急诊医生对收治医院的选择对OHCA患者预后的影响。
分析了2007年至2008年期间在德国多特蒙德市复苏登记处收集的所有患者数据。排除18岁以下、有创伤机制和病历不完整的患者。收治医院分为两组:无经皮冠状动脉介入治疗(PCI)能力的医院和有PCI能力的医院。采用多变量统计分析数据,同时考虑轻度治疗性低温治疗的效果以及收治医院的PCI能力对出院时神经状态的影响。
2007年至2008年期间,多特蒙德市共登记了1109次心肺复苏尝试,其中889次可纳入本研究。889例患者中有360例实现了自主循环恢复(40.5%)。总共889例患者中有282例在转运至医院期间实现了自主循环恢复(31.7%);152例在持续心肺复苏的情况下被转运(17.1%)。在总共434例入院患者中,264例被收治到无PCI能力的医院,170例被收治到有PCI能力的医院。多变量分析表明,对于收治到有PCI能力医院的患者,出院时神经状态良好有显著影响(优势比3.14(95%置信区间1.51至6.56)),与是否接受轻度治疗性低温和/或PCI无关。与收治到无PCI能力医院的患者相比,有PCI能力医院的患者出院时存活的比例显著更高(41%对13%,P<0.001),且在事件发生后1年仍存活的比例也更高(28%对6%,P<0.001)。
OHCA患者收治医院的选择对治疗和预后有显著影响。这种影响与PCI操作和轻度治疗性低温无关。需要进一步分析以确定决定患者预后的可能参数。