Department of Emergency and Critical Care Medicine, Shinshu University School of Medicine, 3-1-1 Asahi, Matsumoto, 390-8621 Japan.
J Intensive Care. 2014 Jun 2;2(1):33. doi: 10.1186/2052-0492-2-33. eCollection 2014.
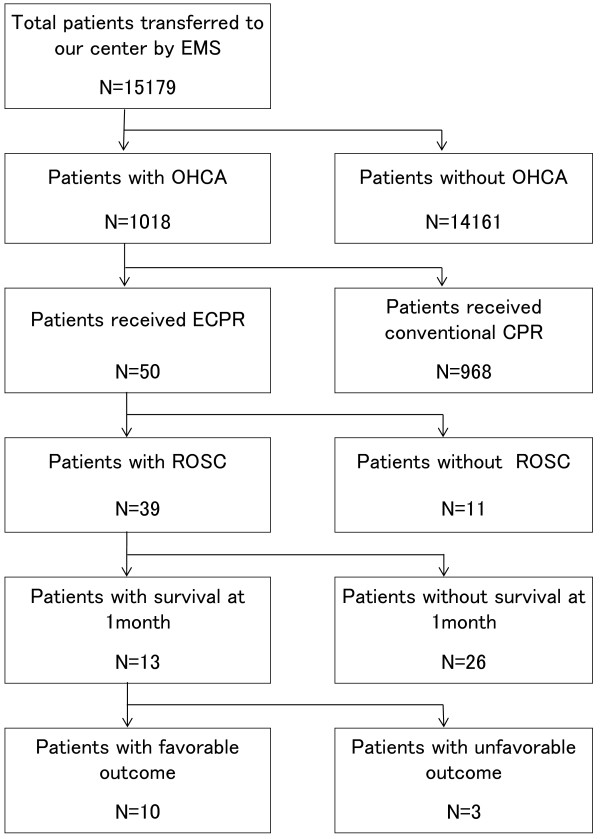
In a rural region with few medical resources, we have promoted the strategy that if an out-of-hospital cardiac arrest (OHCA) patient is likely reversible, he or she should be transported directly from the scene of cardiac arrest to the only tertiary care center where extracorporeal cardiopulmonary resuscitation (ECPR) is readily available. We investigated 1-month survival and neurological outcomes after ECPR in OHCA patients at this center.
We implemented a retrospective review of OHCA patients of heterogeneous origin in whom ECPR was performed. Demographic characteristics, cardiopulmonary resuscitation, ECPR details, and neurological outcomes were evaluated. Cerebral performance categories were used to assign each patient to favorable or unfavorable outcome groups.
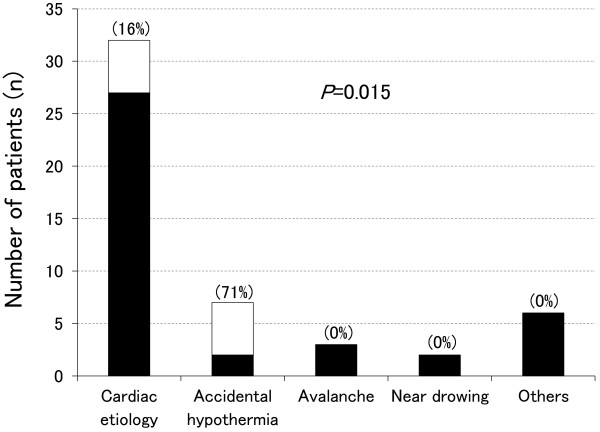
Fifty OHCA patients underwent ECPR. Presumed causes of OHCA were cardiac etiology in 32 patients, accidental hypothermia in 7 patients, and other causes in 11 patients. Overall, 13 patients (26%) survived and 10 patients (20%) had favorable outcomes. Of the 32 patients with OHCA of cardiac origin, 5 patients (16%) had favorable outcomes. Of the seven patients with OHCA of hypothermic origin, five patients (71%) had favorable outcomes. No clinically reliable predictors to identify ECPR candidates were found. However, all nine OHCA patients over 70 years of age had unfavorable outcomes (P = 0.224). In addition, all seven patients who satisfied the basic life support termination-of-resuscitation rule had unfavorable outcomes (P = 0.319).
ECPR can be a useful means to rescue OHCA patients who are unresponsive to conventional cardiopulmonary resuscitation in a rural tertiary care center, in a manner similar to that observed in the urban regions.
在一个医疗资源匮乏的农村地区,我们推行了这样一种策略:如果一名院外心脏骤停(OHCA)患者有可能复苏,应直接将其从心脏骤停现场转运至唯一一家能够立即进行体外心肺复苏(ECPR)的三级医疗中心。我们调查了该中心接受 ECPR 的 OHCA 患者的 1 个月生存率和神经功能结局。
我们对不同来源的接受 ECPR 的 OHCA 患者进行了回顾性分析。评估了患者的人口统计学特征、心肺复苏、ECPR 详细信息和神经功能结局。使用脑功能分类对每位患者进行预后分组,分为有利和不利结局组。
50 名 OHCA 患者接受了 ECPR。OHCA 的推测病因中,心脏病因 32 例,意外低温 7 例,其他原因 11 例。总体而言,13 名患者(26%)存活,10 名患者(20%)预后良好。32 例心脏来源的 OHCA 患者中,5 例(16%)预后良好。7 例低温来源的 OHCA 患者中,5 例(71%)预后良好。未发现可用于识别 ECPR 候选者的可靠临床预测指标。然而,年龄均超过 70 岁的 9 名 OHCA 患者全部预后不良(P=0.224)。此外,满足基本生命支持终止复苏规则的 7 例患者全部预后不良(P=0.319)。
在农村三级医疗中心,ECPR 可作为一种有用的手段来抢救对常规心肺复苏无反应的 OHCA 患者,与城市地区的效果相似。