MRC Clinical Trials Unit, London, UK.
Clin Infect Dis. 2012 Dec;55(12):1707-18. doi: 10.1093/cid/cis797. Epub 2012 Sep 12.
Adult mortality in the first 3 months on antiretroviral therapy (ART) is higher in low-income than in high-income countries, with more similar mortality after 6 months. However, the specific patterns of changing risk and causes of death have rarely been investigated in adults, nor compared with children in low-income countries.
We used flexible parametric hazard models to investigate how mortality risks varied over the first year on ART in human immunodeficiency virus-infected adults (aged 18-73 years) and children (aged 4 months to 15 years) in 2 trials in Zimbabwe and Uganda.
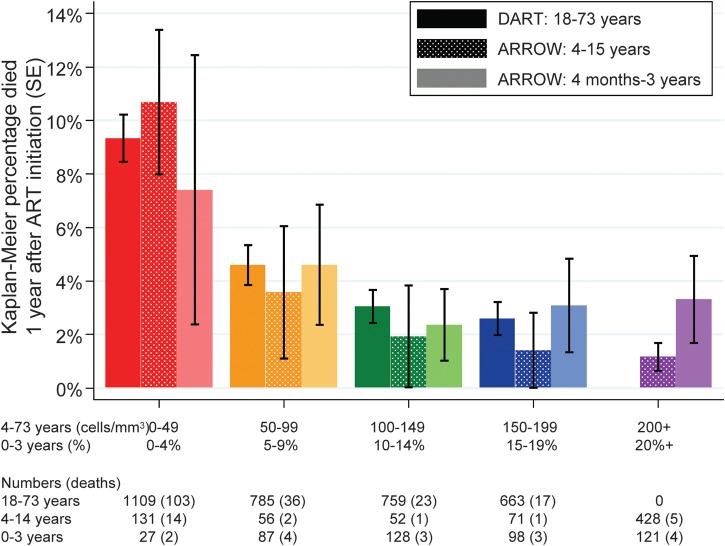
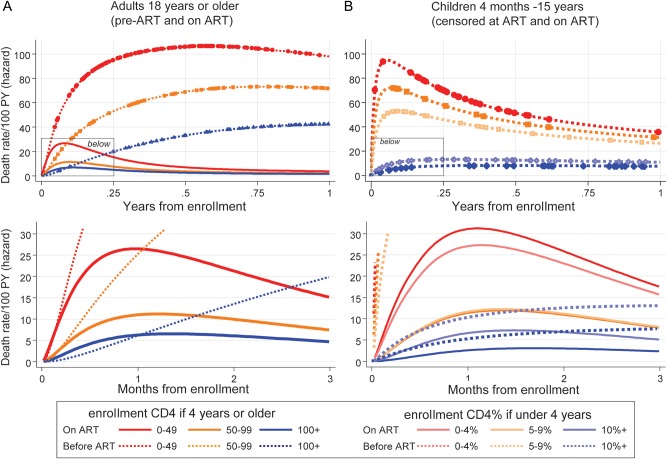
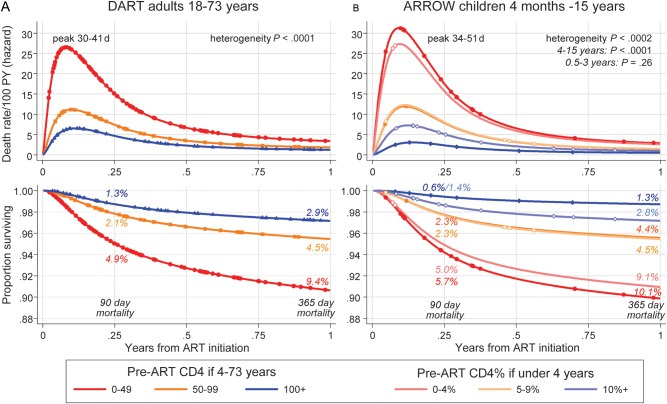
One hundred seventy-nine of 3316 (5.4%) adults and 39 of 1199 (3.3%) children died; half of adult/pediatric deaths occurred in the first 3 months. Mortality variation over year 1 was similar; at all CD4 counts/CD4%, mortality risk was greatest between days 30 and 50, declined rapidly to day 180, then declined more slowly. One-year mortality after initiating ART with 0-49, 50-99 or ≥ 100 CD4 cells/μL was 9.4%, 4.5%, and 2.9%, respectively, in adults, and 10.1%, 4.4%, and 1.3%, respectively, in children aged 4-15 years. Mortality in children aged 4 months to 3 years initiating ART in equivalent CD4% strata was also similar (0%-4%: 9.1%; 5%-9%: 4.5%; ≥ 10%: 2.8%). Only 10 of 179 (6%) adult deaths and 1 of 39 (3%) child deaths were probably medication-related. The most common cause of death was septicemia/meningitis in adults (20%, median 76 days) and children (36%, median 79 days); pneumonia also commonly caused child deaths (28%, median 41 days).
Children ≥ 4 years and adults with low CD4 values have remarkably similar, and high, mortality risks in the first 3 months after ART initiation in low-income countries, similar to cohorts of untreated individuals. Bacterial infections are a major cause of death in both adults and children; targeted interventions could have important benefits.
在接受抗逆转录病毒疗法(ART)的前 3 个月,低收入国家的成人死亡率高于高收入国家,但 6 个月后死亡率更为相似。然而,成人死亡率风险变化的具体模式以及死亡原因很少被研究,也没有与低收入国家的儿童进行比较。
我们使用灵活的参数风险模型,研究了在津巴布韦和乌干达进行的两项试验中,感染人类免疫缺陷病毒的成年(18-73 岁)和儿童(4 个月至 15 岁)在接受 ART 的第一年中,死亡率风险是如何随时间变化的。
3316 名成年人中有 179 人(5.4%)死亡,1199 名儿童中有 39 人(3.3%)死亡;一半的成人/儿科死亡发生在前 3 个月。第 1 年的死亡率变化相似;在所有 CD4 计数/CD4%下,死亡率风险在第 30 天至第 50 天最高,迅速下降至第 180 天,然后缓慢下降。在开始接受 ART 时 CD4 细胞计数为 0-49、50-99 或≥100 个/μL 的成年人中,1 年死亡率分别为 9.4%、4.5%和 2.9%,而年龄在 4-15 岁的儿童中,死亡率分别为 10.1%、4.4%和 1.3%。在 CD4%相同的情况下,开始 ART 的 4 个月至 3 岁儿童的死亡率也相似(0%-4%:9.1%;5%-9%:4.5%;≥10%:2.8%)。在 179 例成人死亡中,只有 10 例(6%)可能与药物有关,而在 39 例儿童死亡中,只有 1 例(3%)可能与药物有关。成人死亡的最常见原因是败血症/脑膜炎(20%,中位数 76 天)和儿童(36%,中位数 79 天);肺炎也是儿童死亡的常见原因(28%,中位数 41 天)。
在低收入国家,开始 ART 后前 3 个月,≥4 岁的儿童和 CD4 值较低的成人死亡率风险非常相似,且非常高,与未接受治疗的个体相似。细菌感染是成人和儿童死亡的主要原因;针对性干预可能会带来重要的益处。