Department of Parasitology-Mycology, Université des Sciences de la Santé, B.P.4009, Libreville, Gabon.
BMC Infect Dis. 2012 Sep 13;12:216. doi: 10.1186/1471-2334-12-216.
Although a substantial decline of Plasmodium falciparum infection is observed in Africa following implementation of new control strategies, malaria is still considered as the major cause of febrile illness in hospitalized African children. The present study was designed to assess the management of febrile illness and to determine the proportion of children with febrile illness hospitalized for primary diagnosis of malaria who had confirmed complicated malaria after implementation of new malaria control strategies in Libreville, Gabon.
Demographic, clinical and biological data from hospitalized children with fever or a history of fever, with a primary diagnosis of clinical malaria, aged less than 18 years old, who benefited from hematological measurements and microscopic malaria diagnosis, were recorded and analyzed during a prospective and observational study conducted in 2008 in the Centre Hospitalier de Libreville.
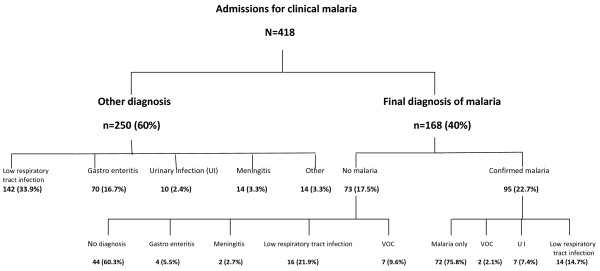
A total of 418 febrile children were admitted at hospital as malaria cases. Majority of them (79.4%) were aged below five years. After medical examination, 168 were diagnosed and treated as clinical malaria and, among them, only 56.7% (n = 95) had Plasmodium falciparum positive blood smears. Age above five years, pallor, Blantyre Coma Score ≤2 and thrombocytopenia were predictive of malaria infection. Respiratory tract infections were the first leading cause of hospitalization (41.1%), followed by malaria (22.7%); co-morbidities were frequent (22%). Less than 5% of suspected bacterial infections were confirmed by culture. Global case fatality rate was 2.1% and 1% for malaria. Almost half (46%) of the children who received antimalarial therapy had negative blood smears. Likewise, antibiotics were frequently prescribed without bacteriological confirmation.
The use of clinical symptoms for the management of children febrile illness is frequent in Gabon. Information, training of health workers and strengthening of diagnosis tools are necessary to improve febrile children care.
尽管在实施新的控制策略后,非洲的恶性疟原虫感染率大幅下降,但疟疾仍被认为是住院非洲儿童发热的主要原因。本研究旨在评估发热性疾病的管理,并确定在加蓬利伯维尔实施新的疟疾控制策略后,因疑似疟疾而住院的发热儿童中,经证实患有复杂疟疾的比例。
2008 年,在利伯维尔中心医院进行了一项前瞻性观察研究,记录和分析了患有发热或发热史、年龄小于 18 岁、接受过血液学测量和显微镜疟疾诊断的住院发热儿童的人口统计学、临床和生物学数据。这些儿童被诊断为临床疟疾,并进行了原发性诊断。
共有 418 例发热儿童因疟疾住院。其中大多数(79.4%)年龄在五岁以下。经过医学检查,有 168 例被诊断为临床疟疾并接受治疗,其中只有 56.7%(n=95)的血涂片阳性。五岁以上、面色苍白、布氏昏迷评分≤2 和血小板减少症是疟疾感染的预测因素。呼吸道感染是住院的首要原因(41.1%),其次是疟疾(22.7%);合并症很常见(22%)。不到 5%的疑似细菌感染经培养证实。总的病死率为 2.1%,疟疾为 1%。近一半(46%)接受抗疟治疗的儿童血涂片阴性。同样,抗生素也经常在没有细菌学确认的情况下开具。
在加蓬,临床症状常用于管理儿童发热性疾病。需要加强信息、培训卫生工作者并改善诊断工具,以提高对发热儿童的护理。