Department of Otolaryngology - Head and Neck Surgery, University of Iowa Hospitals and Clinics, Iowa City, IA 52242, USA.
Hear Res. 2012 Oct;292(1-2):51-8. doi: 10.1016/j.heares.2012.08.007. Epub 2012 Aug 28.
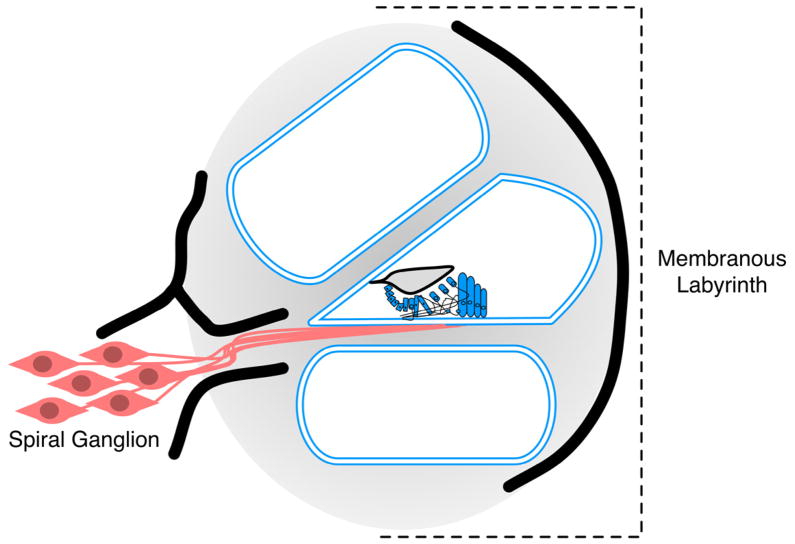
Up to 7% of patients with severe-to-profound deafness do not benefit from cochlear implantation. Given the high surgical implantation and clinical management cost of cochlear implantation (>$1 million lifetime cost), prospective identification of the worst performers would reduce unnecessary procedures and healthcare costs. Because cochlear implants bypass the membranous labyrinth but rely on the spiral ganglion for functionality, we hypothesize that cochlear implant (CI) performance is dictated in part by the anatomic location of the cochlear pathology that underlies the hearing loss. As a corollary, we hypothesize that because genetic testing can identify sites of cochlear pathology, it may be useful in predicting CI performance.
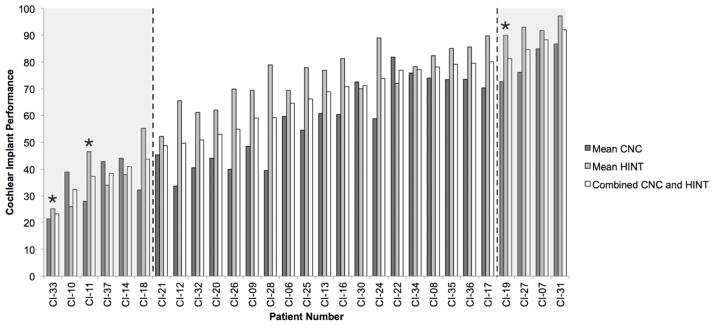
29 adult CI recipients with idiopathic adult-onset severe-to-profound hearing loss were studied. DNA samples were subjected to solution-based sequence capture and massively parallel sequencing using the OtoSCOPE(®) platform. The cohort was divided into three CI performance groups (good, intermediate, poor) and genetic causes of deafness were correlated with audiometric data to determine whether there was a gene-specific impact on CI performance.
The genetic cause of deafness was determined in 3/29 (10%) individuals. The two poor performers segregated mutations in TMPRSS3, a gene expressed in the spiral ganglion, while the good performer segregated mutations in LOXHD1, a gene expressed in the membranous labyrinth. Comprehensive literature review identified other good performers with mutations in membranous labyrinth-expressed genes; poor performance was associated with spiral ganglion-expressed genes.
Our data support the underlying hypothesis that mutations in genes preferentially expressed in the spiral ganglion portend poor CI performance while mutations in genes expressed in the membranous labyrinth portend good CI performance. Although the low mutation rate in known deafness genes in this cohort likely relates to the ascertainment characteristics (postlingual hearing loss in adult CI recipients), these data suggest that genetic testing should be implemented as part of the CI evaluation to test this association prospectively.
高达 7%的重度至极重度耳聋患者不能从人工耳蜗植入中受益。鉴于人工耳蜗植入的高手术植入和临床管理成本(超过 100 万美元的终身成本),前瞻性地识别预后最差的患者可以减少不必要的手术和医疗保健费用。由于人工耳蜗植入绕过了膜迷路,但依赖于螺旋神经节发挥功能,我们假设人工耳蜗植入(CI)的性能在一定程度上取决于导致听力损失的耳蜗病变的解剖位置。因此,我们假设,由于基因测试可以识别耳蜗病变的部位,它可能有助于预测 CI 的性能。
研究了 29 名患有特发性成人后天重度至极重度听力损失的成年人工耳蜗植入者。使用 OtoSCOPE(®)平台对 DNA 样本进行基于溶液的序列捕获和大规模平行测序。该队列分为三组 CI 性能组(良好、中等、差),并将耳聋的遗传原因与听力数据相关联,以确定是否存在基因对 CI 性能的特定影响。
在 29 名个体中的 3 名(10%)确定了耳聋的遗传原因。两名预后不良的患者携带 TMPRSS3 基因突变,该基因在螺旋神经节中表达,而表现良好的患者携带 LOXHD1 基因突变,该基因在膜迷路中表达。全面的文献回顾确定了其他表现良好的患者存在膜迷路表达基因的突变;而表现差与螺旋神经节表达基因相关。
我们的数据支持这样的假设,即在螺旋神经节中优先表达的基因突变预示着 CI 性能差,而在膜迷路中表达的基因突变预示着 CI 性能好。尽管在该队列中已知耳聋基因的突变率较低可能与确定特征(成年人工耳蜗植入者的后天性听力损失)有关,但这些数据表明,应该将基因测试作为 CI 评估的一部分来前瞻性地测试这种关联。